
Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Most discussed topics
Brands & references
No brand mentions extracted.
Est. Listeners
Insufficient chart data. Estimates will improve as the show charts.
- Per-Episode Audience
Est. listeners per new episode within ~30 days
N/A🎙 ~2x weekly·47 episodes·Last published 2mo ago - Monthly Reach
Unique listeners across all episodes (30 days)
N/A - Active Followers
Loyal subscribers who consistently listen
N/A
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
From 1 epsHost
Recent guests
No guests detected in recent episodes.
Recent episodes
Burnout De-escalation and Damage Limitation in Neurodivergent Menopause 💐 🎥 🎧
Apr 26, 2026
30m 47s
The Divergent Menopause Q&A: Tell Us Your Story!
Apr 17, 2026
13m 13s
You’re Not “Dry.” You’re Underinformed.
Mar 31, 2026
17m 00s
(Live) Perimenopause as a Burnout Accelerant 🎥🎧💕
Mar 27, 2026
1h 40m 08s
Who Taught Us Not to Know Our Bodies? 🎥💕🗝️
Mar 17, 2026
19m 05s
Social Links & Contact
Official channels & resources
Official Website
Login
RSS Feed
Login
| Date | Episode | Topics | Guests | Brands | Places | Keywords | Sponsor | Length | |
|---|---|---|---|---|---|---|---|---|---|
| 4/26/26 | 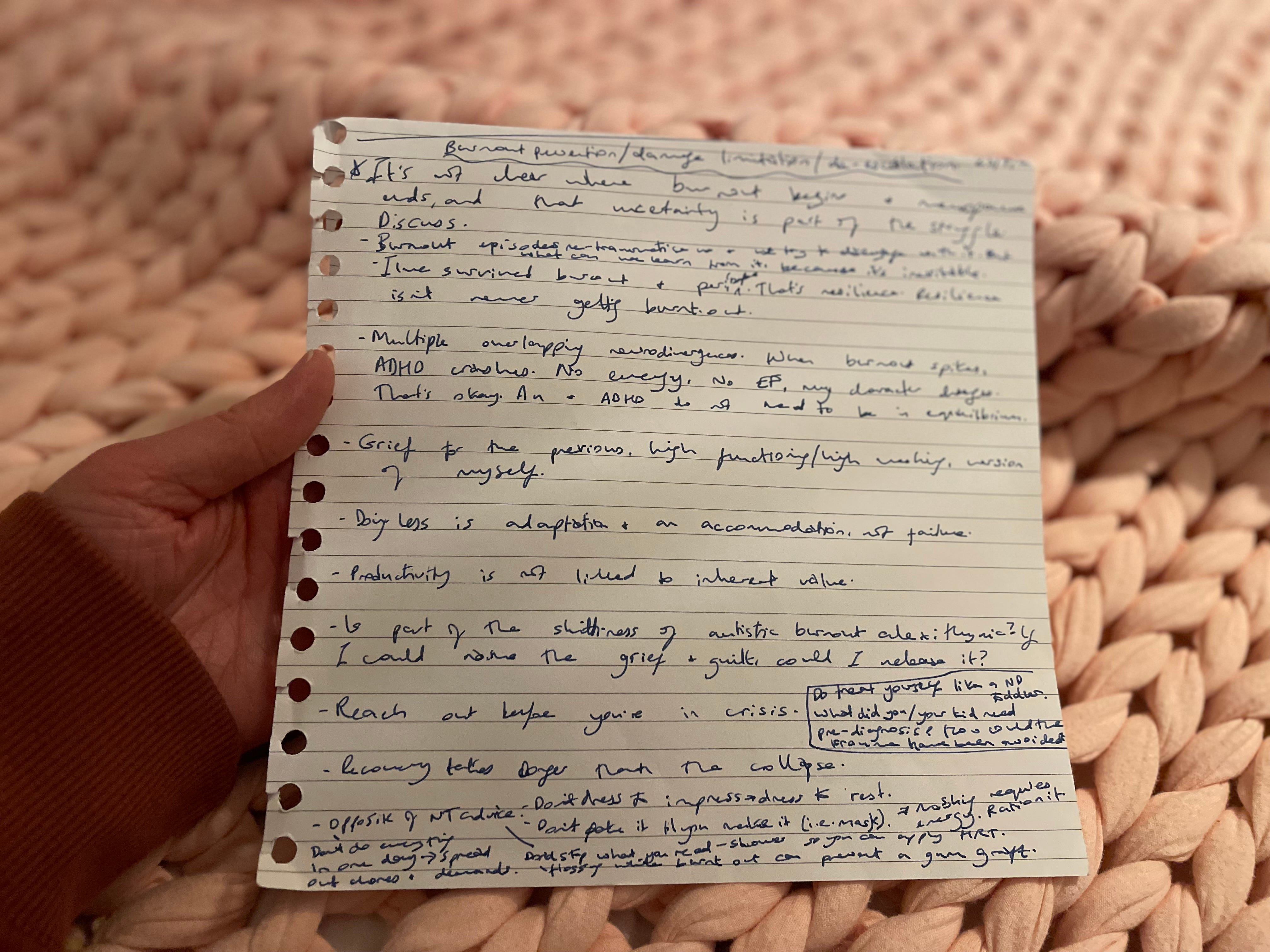 Burnout De-escalation and Damage Limitation in Neurodivergent Menopause 💐 🎥 🎧✨ | neurodivergentburnout+5 | — | — | — | burnoutneurodivergent+8 | — | 30m 47s | |
| 4/17/26 |  The Divergent Menopause Q&A: Tell Us Your Story! | In this episode, I’m relaunching The Divergent Menopause Q&A: a community-driven series sharing real lived experiences of neurodivergent menopause.This is an open invitation to contribute your story.We talk about:Why neurodivergent menopause is so underrepresentedThe risks of silence and lack of supportThe importance of lived experience alongside researchWhat to expect if you take partIf you’ve ever felt unseen, dismissed, or alone in this stage of life this space is for you.Take part in the Q&A: The Divergent Menopause Q&AContent note: Mentions of mental health and suicide risk.Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer (AuDHDer), and a surgical menopause survivor. I write Divergent Menopause to share what many of us are never told until we have to find out the hard way.Thanks for joining me on this wild midlife ride! 🎢The Divergent Menopause Q&ATell us your story!Hi All,If you have been here a while you might remember that I used to host an interview series called Auti Peri Q&A. You can find all the interviews here. When I changed the name of my publication to Divergent Menopause I knew that I would want to share the voices of others because if you’ve met one menopausal neurodivergent person, you’ve met one menopausal neurodivergent person.My own menopause story is uniquely bleak, and I want us all to know about other ways our neurokin are surviving this often challenging life phase. My goals are always to share experiences and build community around neurodivergent menopause.I am now relaunching the Q&A series under the name The Divergent Menopause Q&A, and am opening it up to all people who identify as neurodivergent with lived experience of the menopause transition!Completed Q&As will be published here and, emailed out to my subscribers. Respondents can be anonymised when it goes online, although I will need an email address to contact you and make sure you are happy with the final edit.Your email address will not be shared in the post, nor shared with any third parties. Without a contact email address to reach out to you, I will be unable to publish your Q&A.I would LOVE to share your neurodivergent menopause story! It doesn’t need to be remarkable or dramatic.We already know from research that the rate of suicide is higher for neurodivergent midlife people transitioning through menopause compared to the neurotypical population.We have no time to waste in sharing our experiences, and getting the message across that perimenopause and hormonal fluctuations can affect neurodivergent people in a more extreme and potentially harmful way than the neurotypical population. Whilst also showing that this isn’t the case for all neurodivergent people.I want this feature to be inclusive of all races and genders of people who experience the menopausal transition. White cisgender women dominate the narrative, so if you or someone you know from a minority demographic group would like to participate in The Divergent Menopause Q&A Series, please reach out to me.I aim to diversify the message and be representative of all neurodivergent peri/menopausal people.Below is the information you will find directly on The Divergent Menopause Q&A when you click this link, followed by the 12 questions, so you know what to expect.Thank you for being here.This Q&A is part of a series sharing the lived experiences of neurodivergent people going through menopause and perimenopause. You may already be familiar with my previous interview series, The Auti Peri Q&A.Neurodivergent perimenopause is a highly individual, dynamic and sometimes prolonged life stage represented by fluctuations in physical, psychological and cognitive symptoms that can be different for everyone.None of us should have to feel alone at this time of our lives.By sharing your story, you are helping to:💕 Raise self-advocacy as a community effort, not just an individualised responsibility💕 Contribute meaningfully and anecdotally to the growing body of work and research into neurodivergent menopause💕 Empower our unified voiceWe have no time to waste in sharing our lived experiences, and getting the message across that perimenopause and hormonal fluctuations can affect neurodivergent people in a more extreme and potentially harmful way than the neurotypical population. Whilst hopefully also showing that this isn’t the case for all neurodivergent people.On the next page I will explain my Q&A process.Thank you for trusting me with your story.How to Q&ABy sharing your experience, you are helping to build understanding, challenge silence, and make this transition more visible for others.On the next page you will be asked to provide some information about yourself, and to upload a photo that you would like to accompany your published Q&A post.On the following pages there are twelve open ended questions and prompts where you are invited to share your neurodivergent menopause experience in your own words. There is no right way to answer these questions. You can write as much or as little as feels manageable.But please do provide as much detail as possible because this is not a survey. The more information you share, the richer your published Q&A post will be, and the more other people can learn from your lived experience.Your responses will be treated with care and respect. I may lightly edit for clarity and flow, while keeping your voice and meaning intact. Nobody else has access to your responses, and I will be notified when you submit the completed Q&A. I will then go through a formatting process to prepare your post on Substack, invite you to be a guest writer, and send you the draft link for your approval.When we are both happy with it we will decide when to schedule its release. On that day, your Q&A post will be emailed to my subscriber list, and published on Divergent Menopause as part of an ongoing series.If answering the questions all feels like too much, please stop. You are under no obligation to complete the Q&A once you start, and I will totally understand if you change your mind.There is no time limit, so you can return to it in the future if now is not a good time for you.Please prioritise your own mental wellbeing at all times.Any questions, insights or feedback? You are welcome to contact me via Substack DMs or email me at: divergentmenopause@gmail.comLet’s go!The Questions:Q1. Your perspectiveWhat does “neurodivergent menopause” mean to you?Take your time, there’s no need to summarise.Q2. When things changedWhen did your neurodivergent menopause symptoms start and what were/are they? You can include physical, emotional, sensory, cognitive, social, and/or sexual changes.Q3. Menopause healthcareWhat happened if/when you presented with neurodivergent menopause to a healthcare professional?Q4. Treatment and symptom managementWhat has your treatment protocol been in managing your neurodivergent menopause?You can include medical, alternative, herbal, therapeutic, surgical, spiritual, diet, exercise etc.Q5. Daily impactHow has your everyday life and sense of self been impacted by neurodivergent menopause? You can include your caring/employment responsibilities, hobbies, relationships etc.Q6. ChallengesAre there things that make or have made your menopause transition especially difficult for you as a neurodivergent person? If so, what kinds of things?Q7. What has helpedWhat kinds of services, treatments, resources or supports have you found most helpful?Q8. Treatment and symptom managementAre there things that could make or could have made your menopause transition easier for you as a neurodivergent person? If so, what kinds of things?Q9. What’s been hardestWhat has felt most difficult or overwhelming?Q10. Support where you liveWhat support, services or resources exist where you are?How accessible are they?Q11. What you want people to understandWhat do you wish more people understood about neurodivergent menopause?Q12. Anything elseIs there anything else you’d like to share? Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 13m 13s | ||||||
| 3/31/26 |  You’re Not “Dry.” You’re Underinformed. | There is a common menopause-related condition that can cause tearing, burning, recurrent urinary tract infections(UTIs), loss of sexual function and many other symptoms. And it does not improve with time.Yet most people have never heard of it. Even our doctors!If you’ve ever been told it’s “just thrush,” “just dryness,” or “just part of getting older”, then this is for you.Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer (AuDHDer), and a surgical menopause survivor. I write Divergent Menopause to share what many of us are never told until we have to find out the hard way.Thanks for joining me on this wild midlife ride! 🎢TL;DR:Genitourinary Syndrome of Menopause (GSM) is a common but underdiagnosed condition that can cause tearing, burning, recurrent UTIs, and loss of sexual function. And it does not improve with time.Many people (including doctors) mistake it for infections or “normal ageing.”Effective treatment exists but most of us are never told.2025 changed everything for meFor me personally, it was the year of my life saving gynaecological operation that immediately put me into surgical menopause, aged 44. If you have been here a while you may already know that I had a total hysterectomy with bilaterel salpingo-oopherectomy i.e. my uterus, cervix, fallopian tubes and ovaries were removed. YAY!! This was for several reasons including thickening of my endometrium (lining of the womb), progesterone intolerance, premenstrual dysphoric disorder (PMDD), chronic pelvic pain, and prolonged mental health issues caused by the hormonal flux of perimenopause. After the initial recovery time, which was blissful bedrest on Codeine, building LEGO and binge watching Taskmaster for a couple of months, I am glad to report that my mood is finally stable. And now with the use of systemic add-back hormone replacement therapy (HRT)/menopause hormone therapy (MHT), my life is back on track, and my hormonal flux has been eliminated.But my surgery was just the beginning of my menopause. It surgically ended my horrendous perimenopause, but I have sadly not been spared the full post-menopausal array of hormonally depleted horrors.Yes, I am 44. No, I am not too young to have Genitourinary Syndrome of Menopause (GSM).Genitourinary syndrome of menopause isn’t all about dryness, and “dryness” isn’t even what we think it is. It isn’t wiping after using the toilet, and shredding the paper on your sandpaper-like skin. Dryness is more like labial tears that don’t heal, burning that can’t be soothed, and an itch that isn’t thrush. And that is only for starters…I am not judging anyone for thinking that dryness only means that your vulva feels parched and sex hurts. Lubricating might offer temporary relief but it is no cure. This is a lot and it has all been a steep learning curve for me. There is so much I didn’t know. I didn’t know even after I had shown to my own labial tear to my usual doctor when I was 39 or so, and he had prescribed an antifungal and antibacterial cream that I diligently applied. Even after I then went back because it hadn’t healed, and showed it to yet another doctor at the surgery, and she described the skin as “friable” (which I learned meant extremely fragile skin), and prescribed the same medication, on the wrong assumption that it must have been a particularly stubborn fungal infection. I was still none the wiser about GSM.And neither were the doctors treating me.Has anything like this ever happened to you?I would genuinely like to know how many of us were persistently treated for infections that never existed.It wasn’t until I first saw my menopause specialist doctor months, perhaps even a couple of years, later that I began to learn what was really happening to my body. As we live in distant parts of Aotearoa New Zealand, appointments with my menopause doctor are usually remote via telemedicine video or phone calls, and graphic anatomical photos are sent over a secure medical online portal to inform assessments. So when my tear wasn’t healing I eventually sent a photo of it to my menopause doctor. She reported that the tissues looked pale and inflamed. Immediately I was prescribed the correct treatment (and I hurriedly deleted the photos from my phone before anyone else saw them..!)Although my doctor didn’t call it “genitourinary syndrome of menopause”, it didn’t take me long to bolt down the dry, pale and friable rabbit hole of doom. 🕳️And what was the miracle cream that I still use twice a week, and will need to be prised from my cold dry dead hands? Vaginal oestrogen cream! Here is a post from the Divergent Menopause (formerly The Autistic Perimenopause: A Temporary Regression) archives way back in 2024 when GSM was a agonisingly brand new and thrilling concept to me:What else happened in 2025?On a much more significant scale than my hysterectomy, a groundbreaking step was made by the United States medical authorities. Yet this news completely went under my radar until a few weeks ago, when I listened to a podcast episode from April 2025, where urologists Kelly Casperson, MD and Rachel Rubin excitedly announced the new guidelines on genitourinary syndrome of menopause. I learn more from this discussion with every listen. Feeding off their energy, I went straight into hyper ADHD mode and developed an intense interest in this little known, painfully taboo, yet extremely common syndrome that has been affecting me - and possibly you too? - for years. Last year, the American Urology Association (AUA), Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) and American Urogynecologic Society (AUGS) jointly published the Genitourinary Syndrome of Menopause: AUA/SUFU/AUGS Guideline (2025). Six years in the making, this guideline was written to provide clinicians with the necessary information to identify, diagnose, counsel and treat GSM.So what symptoms count as GSM? Probably not what you think, and you may already have some of them. Brace yourself…Vulvovaginal symptoms* Dryness* Burning * IrritationUrinary symptoms* Urgency* Frequency* Dysuria (pain, discomfort or burning whilst urinating)* Recurrent urinary tract infections (UTIs)Vulvovaginal and urinary effects of menopause combined cause the sexual symptoms:* Dyspareunia (painful intercourse)* Bleeding during intercourse* Broader impacts on sexual function: reduced libido, reduced arousal and reduced orgasmPhysical changes of GSM:* Labial atrophy* Reduced moisture* Introital stenosis (narrowing/shortening/closing/loss of flexibility of vagina and vaginal opening due to scar tissue) leads to pain in sex, discomfort during pelvic exams and difficulty using tampons* Clitoral atrophy. CLITORAL ATROPHY!!??Vaginal surface may be:* Friable (tissue that is easily irritated and more prone to inflammation, bleeding and tearing)* Hypopigmented (pale skin)* Petechiae (pinprick sized red or purple spots on the skin from fragile capillaries bursting)* Ulcerations * Tears in the skin (from personal experience, I can report that this burns like a biatch, and doesn’t heal without vaginal oestrogen)Urethral (the hole you pee from) findings:* Caruncles (benign vascular growth on outside of the urethra)* Prolapse (a pelvic organ loses it’s support and falls down into the urethra)* Polyps This list is not comprehensive, there are other symptoms that I don’t know about yet. Please share in the comments if you know of others that I have missed. Did you know that the term “Genitourinary Syndrome of Menopause” doesn’t even cover the entirety of this issue, nor the time in your lifespan when these GSM symptoms can occur?Genitourinary symptoms occur during other life stages of hormonal flux including pregnancy, postpartum, when taking hormonal contraceptives, and whilst breastfeeding. I am still quaking from this news. I breastfed both my boys until they were four years old because, before my perimenopause tried to kill me and I needed a medical treatment pathway to preserve my life, I was a super crunchy, all natural, hippie Mama. Now in hindsight I think that my fellow woke lefty greeny attachment parenting Mama and baby community were all undiagnosed neurodivergents too. I wouldn’t have wanted it any other way! And before I 100% wanted babies I 100% didn’t want babies, and so I spent decades on the contraceptive pill, contraceptive injections and contraceptive implants. Is it any wonder that my poor vag is now utterly wrecked due to a lack of oestrogen through so many years of my life? Yet we get told that the stitches, tears and birth injuries are the worst issues of early motherhood and that, whatever happens, we are lucky as long as we have birthed a “healthy” baby. If only I knew then what I know now… Someone should have handed me a prescription for vaginal oestrogen there and then! Imagine if the midwives handed it out immediately after birth? It would have soothed my tattered vagina stitches, I reckon.This is our time to get informed. When we know better, we can take better care of ourselves.During the ‘You Are Not Broken’ podcast episode, recorded on the day of release of the new (at the time) GSM guidelines in 2025, Dr Rachel Rubin said:“… it is bold, it is simple, it is unapologetic, it is evidence-based, and it is very, very clear that vaginal hormones are absolutely preventative of urinary… tract infections, help with pain with intercourse, help with overactive bladder and urinary urgency. They are safe to take if you have breast cancer history, family history of breast cancer, history of blood clots.“They are safe, and they are… lifelong therapies. They are chronic therapies that should be used…“… This is urinary frequency and urgency, recurrent urinary tract infections which kill people. It is pain with sex, dryness, muted orgasms, absent arousal. It is, it is, and it doesn’t get better with time.“Sometimes hot flashes get better. But as your audience knows, the genitourinary symptoms do not get better for most people.”From You Are Not Broken: 315. BONUS - Genitourinary Syndrome of Menopause Guidelines released today!, 29 Apr 2025If you aren’t already using vaginal oestrogen, then why not? There is so much to be gained. It is so much better to prevent GSM than to have to suffer with insidious symptoms unnecessarily.If you recognise yourself in this, you are not broken, you are underinformed. And you deserved to know all this sooner. This is the kind of information I wish I had had years earlier!If this post helped you understand something about your body that no one has explained before, you can support this work becoming a patron as a paid subscriber.Cheers,Paid subscribers make it possible for me to keep researching, writing, and sharing the information many of us are missing. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 17m 00s | ||||||
| 3/27/26 |  (Live) Perimenopause as a Burnout Accelerant 🎥🎧💕 | If you’ve ever felt like your brain stopped working in neurodivergent midlife, this discussion may explain why.Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer (AuDHDer), and I have recently had a hysterectomy. As a neurodivergent perimenopause and PMDD survivor, I offer peer support and share knowledge on how to make it through the hard times.Thanks for joining me on this wild midlife ride! 🎢Thank you to Marie-Christine Oliver for this is fascinating and enriching chat!So many brilliant people joined us live and we are so grateful for your contributions in the chat, as well as having you all there with us. It was intense so people dipped in and out.For accessibility, the video has closed captions, the transcript is available within this post, and you can listen to an audio only version if preferred.It was a long one (we went 40 minutes over our scheduled hour - ADHD much?), but we covered all the things. Well, we tried to!We even completed the Meno-D rating scale to detect depression in menopause together which is one of my favourite supports in my menopausal transition, along with my cats, and my vaginal oestrogen cream. And yes, I mentioned clitoral atrophy because we should know about these things!⚠️ Content warning for talk of suicidality, disordered eating, mental health hospital stays, early menopause, IVF, medical gaslighting, misdiagnosis, loss of career/function/sense of self, involuntary unmasking, and clitoral atrophy.TL;DRead/Watch/Listen (AI generated)Perimenopause can act as a burnout accelerant for neurodivergent women—especially those with ADHD and autism—because hormonal changes destabilise already overworked nervous systems.This often leads to:* Sudden loss of masking ability* Cognitive decline and emotional dysregulation* Misdiagnosis and medical gaslighting* Identity collapse and increased suicidality riskThe conversation highlights a critical gap: research, language, and clinical understanding are lagging far behind lived experience.⏱️⏱️ Full Timestamped Summary (AI generated)00:00 – Intro (chaotic, human start) Live recording begins; Sam introduces the topic and guest Marie-Christine Oliver.02:00 – Core concept Perimenopause as a burnout accelerant for neurodivergent nervous systems.03:30 – Lived experience IVF, early perimenopause, nervous system collapse, career loss, suicidality, late diagnosis.06:30 – The biology Estrogen supports dopamine + serotonin → drop creates a double neurological hit.07:00 – Masking collapse Sudden loss of ability to cope → meltdowns, shutdowns, dysregulation.08:00 – Cognitive decline Brain fog, memory loss, speech issues → often mistaken for dementia.10:00 – HRT explained A buffer, not a cure; reduces extremes but doesn’t fully restore capacity.13:00 – Mental health risks High rates of suicidality; symptoms often misunderstood or misdiagnosed.15:00 – Research gaps Little to no research on ADHD + menopause or AuDHD.20:00 – Key insight Menopause = point where masking becomes impossible.22:00 – Quadruple empathy problem Breakdown between patient + doctor + neurotype + menopause context.26:00 – Medical gaslighting Symptoms dismissed or mislabelled → confusion + self-doubt.28:00 – Identity collapse Loss of career, function, and sense of self.31:00 – Compounding pressures Parenting, aging parents, chronic illness, hormones—all at once.33:00 – Diagnosis aftermath Labels accumulate; identity becomes deficit-based.36:00 – Menod tool introduced A scale for identifying menopausal depression.40:00 – Why the tool matters Captures real-life impact; useful for self-advocacy.42:00 – Energy depletion Extreme fatigue; even basic tasks feel impossible.43:00 – Paranoid thinking Workplace anxiety, social fear; blurred line between perception and reality.45:00 – Irritability / rage Outbursts, meltdowns → nervous system overload, not personality.47:00 – Self-esteem collapse Ranges from self-doubt to suicidality.49:00 – Hospitalisation Can help or harm; highlights systemic inequalities.50:00 – Social isolation Disconnection even when not alone.52:00 – “What is normal?” Tools often based on neurotypical assumptions.54:00 – Anxiety escalation Chronic nervous system dysregulation. 56:00 – Physical symptoms Pain, illness, unexplained issues tied to hormones + stress.58:00 – Sleep disruption Creates worsening feedback loops.60:00 – Body changes Weight, metabolism, physical identity shifts.62:00 – Libido changes Under-discussed but significant impact.64:00 – Memory + focus issues Deeply distressing; often misinterpreted as cognitive decline.66:00 – Symptom accumulation Multiple high scores = severe functional impact.68:00 – Whole-life impact Work, relationships, parenting all affected.70:00 – Why systems fail Healthcare treats symptoms separately, not holistically.72:00 – Forced self-advocacy Individuals must piece everything together themselves.74:00 – Grief Loss of self, identity, and capacity.76:00 – Burnout cycles Push → crash → partial recovery → repeat.78:00 – Lifelong overcapacity Perimenopause exposes unsustainable patterns.80:00 – Lack of prevention No warning, no preparation, no roadmap.82:00 – What could have helped Earlier diagnosis, awareness, and reduced pressure.84:00 – Systemic gaps Research, healthcare, and workplaces all lagging.86:00 – Community importance Peer conversations filling the gap.88:00 – Reframing Not failure → biological + neurological reality.90:00 – What’s needed next Research, integrated care, recognition.92:00 – Hope (with nuance) Improvement possible, but not full restoration.94:00 – Ongoing vulnerability Need for pacing, boundaries, nervous system care.96:00 – Final reflections This is widespread and under-recognised.98:00 – Closing Validation, connection, and shared understanding.100:00 – EndResources:Meno-D: A rating scale to detect depression in menopauseThe conversations we’re having here are filling a gap that research and healthcare still haven’t caught up with. If this work matters to you, consider becoming a paid subscriber to support it.Thank you to everyone who tuned into my live video! Join me for my next live video in the Substack app. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 1h 40m 08s | ||||||
| 3/17/26 |  Who Taught Us Not to Know Our Bodies? 🎥💕🗝️ | Episode TitleWhy So Many Women Don’t Know Their Own AnatomyEpisode DescriptionIn this conversation, Sam Galloway from Divergent Menopause speaks with Amber Horrox, creator of Warrior Within, about body literacy, menstrual shame and the long shadow of medical misogyny.Many women grow up knowing the names of internal reproductive organs — uterus, ovaries, fallopian tubes — yet struggle to name the external anatomy of their own bodies. Euphemisms, silence and shame mean that even describing symptoms to a doctor can be difficult.Sam and Amber explore:• Why women are rarely taught accurate anatomical language• How euphemisms create barriers in healthcare• The messaging around menstruation and “pushing through” pain• The impact of religious and fear-based sex education• Surgical menopause and chronic pelvic pain• Integrating medical, holistic and embodied approaches to healing• Reclaiming safety and agency in our bodiesA note on languageThis conversation uses the word "women" in places when discussing anatomy, menstruation and menopause. These experiences are not limited to one gender, and people of multiple genders may share them. The language here reflects the conversational nature of the discussion rather than an attempt to exclude anyone whose body or lived experience is part of this topic. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 19m 05s | ||||||
| 3/13/26 |  The Autism Establishment Has a Problem | The recent debate sparked by autism researcher Uta Frith has exposed a growing divide between traditional autism research and autistic lived experience.As more adults identify as autistic and the autism spectrum continues to expand, an increasingly urgent question emerges:Who gets to define autism?Researchers? Clinicians? Or autistic people ourselves?Read the full article on Substack: Divergent MenopauseDirect link to the essay postIn this episode, I unpack the controversy surrounding recent interviews with Professor Dame Uta Frith and reflect on what the debate reveals about the past, present, and future of autism research.Drawing on my own experiences as an autistic ADHDer (AuDHDer), parent of autistic children, and survivor of perimenopause, PMDD and surgical menopause, I explore why many autistic people feel triggered by this discussion, and why autistic voices must be central in conversations about autism.In this episode• The controversy surrounding recent interviews with autism researcher Uta Frith• Why some researchers believe the autism spectrum has become “too wide”• The growing divide between traditional autism research and autistic lived experience• Why masking, sensory needs, and late diagnosis are still debated• How generational views of disability shape autism discourse• The rise of autistic-led research and advocacy• Why many autistic people feel distrustful of traditional research models• The urgent need for research that improves autistic quality of life• Future research questions that could genuinely help autistic peopleTopics discussedAutism research, Neurodivergence, Late autism diagnosis, Masking and autistic burnout, Medical misogyny, Self-diagnosis, The social model of disability, The double empathy problem, Neurodivergent mental health, Autistic menopauseAbout the hostSam Galloway (she/her) is an autistic ADHDer (AuDHDer), writer, and creator of Divergent Menopause.Following her own experiences of neurodivergent perimenopause, PMDD, and surgical menopause, Sam writes and speaks about the intersections of autism, neurodivergence, hormones, and midlife mental health.Her work focuses on peer support, advocacy, and helping neurodivergent people navigate difficult transitions.Content noteThis episode includes discussion of:• medical gaslighting• medical misogyny• mental health services• suicide and suicidal ideationPlease take care while listening.Discussion questionsThis topic has sparked huge debate online, and I’d love to hear where listeners land:• What do you think the biggest gap is between autism research and autistic lived experience?• Have you ever encountered professionals who dismissed masking or sensory needs?• What areas of autism research do you think deserve more attention?Support the publicationIf this episode resonated with you, consider becoming a paid supporter of Divergent Menopause.This publication runs on a patron membership model, and paid subscribers help fund independent writing and advocacy centred on neurodivergent lived experience. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 30m 55s | ||||||
| 2/14/26 |  The Quadruple Empathy Problem | Hello and welcome to Divergent Menopause with Sam Galloway.Today I'm going to read to you the quadruple empathy problem.Autism, ADHD, menopause, and why we are still the ones expected to adapt.Empathy.According to the Cambridge Dictionary,the definition of empathy is the ability to share someone else's feelings orexperiences by imagining what it would be like to be in that person's situation.Empathythe ability to share someone else’s feelings or experiences by imagining what it would be like to be in that person’s situationSource: Cambridge DictionaryThis Elder Millennial vividly recalls standing in front of the bathroom mirror in my locked family bathroom, aged 7 or 8 or so. Forcing tears to stream from my eyes, my crying voice rasping, feeling the hot slime from my sinuses dripping down the back of my throat, I didn’t feel sadness. Perhaps we can grow out of alexithymia, but the act of crying on cue did not prompt emotion. Reflected back to me in the mirror was a girl who cried, smiled, and laughed at all the wrong times. Many hours were spent alone learning to morph my face to look how it was expected of me.“Too much”, “not enough”, “too sensitive” and “insensitive”, were some of the labels attached to me whenever my childhood response was perceived to be misaligned with the social expectation. Learning the rules of emotional expression was arduous and exhausting. Watching the neurotypical girls whisper about me, then trick me into thinking they were my friends before not long later calling me fat, ugly and ginger, was my daytime schooling.Where was their empathy for me?Burnout regularly ensued.Life was endlessly confusing. For reasons still unclear to me, as a girl screaming and crying in pain when I was injured and hurting was deemed over the top. Yet silently sobbing myself to sleep was apparently fine. I learnt that as long as I could hide my emotions from others, I was safe. The agonising intensity of my emotions was not for public consumption, and my pain and anguish was supposed to be kept private.Crying into the mirror, was an instinctual exercise in social masking. Self-set homework was studied only by the special girls like me, in secret, whilst everyone else got on at home with learning more traditionally academic subjects, and playing with easily found and kept friends. My social skills learning was autodidactic in my early years, but would pay off in time when I took it upon myself to achieve an upper second-class honours degree Bachelor of Science in Psychology.The classic Psychology undergrad degree A.K.A. the neurodivergent thinking woman’s endeavour to cognitively grasp concepts behind individual and collective human thoughts, motivations, neurology and behaviours. Including (neurotypical) empathy. Using our strengths of curiosity, pattern recognition and intellect, we endeavour to compensate for the neurodevelopmental lagging skills that made too many of our childhoods a misery.The unrelenting stereotype of neurodivergent people is that we cannot comprehend the emotions of others, never mind be able to empathise with them. It would still be two decades before my autism and ADHD were identified.Despite our extreme efforts to performatively show our emotions in a dignified, standardised and socially acceptable manner, many female and AFABs pre-diagnosed autistic, ADHD and AuDHD can also gaslight ourselves into thinking that we can’t be neurodivergent. How can we be neurodivergent when we show too much emotion, rather than none at all? Our emotional dysregulation can trigger us to weep, and seeing such intense public displays of empathy can make other people uncomfortable.Neurodivergent empathy looks different.But our late identification has prompted family members and society at large to think that we are just jumping on the “latest trend” of autism and ADHD.For those of us who are exquisitely high masking and often with co-occuring giftedness, the assumption is that we can empathise in a neurotypical way, but we choose not to. Too often, we are regarded as arrogant, manipulative, and over- or under- performative.When we eventually receive a diagnosis, having fought a lifelong battle to fit in with the people who love us the most yet understand and accept us the least, it becomes clear that neurotypicals also have difficulty showing us empathy.Our emotions look different.Our empathy looks different.Many late diagnosed neurodivergent women and AFABs, consider ourselves to be deep empaths. For decades, we have masked our emotional intensity, and yet we are often the first to donate to worthy causes and to cry at distressing world news stories. The challenge for us isn’t whether or not we can respond emotionally to others. The challenge for us is self-regulating our emotional responses. When the intensity of our emotional responses is socially unacceptable, we are labelled “too much” and/or “not enough”.Sobbing in work meetings.Melting down during minor disagreements.Shutting down when newly bereaved.Our emotional intensity sets us apart from the majority. To me, this is an advantage to being neurodivergent. But we hide it, moderate our emotional responses, and stop our faces from giving us away, in order to avoid rejection.When the societal norm is to visibly empathise swiftly then move on, our deep empathy is feared and misunderstood. Public crying is deemed shameful, and being told to “grow up” as kids really meant “keep it to yourself”. Hiding our pain doesn’t stop us from feeling it.We made it our mission to pass for normal, and we were picked apart regardless.Our natural response as neurodivergents is pathologised as emotional dysregulation, and we are medicated, therapised and/or shunned to obscure our differences from the world.Many of us learn to shield ourselves from our emotional triggers, for example, by actively avoiding live footage broadcasts of global catastrophes, and the effects of their aftermath.Other neurodivergents may enter politics, education and other influential institutions to try and change systems from the inside in a bid to improve life chances for all, reverse the climate crisis and drive other social justice causes that they empathise with deeply.By midlife, we have learnt to mask and moderate our neurodivergent empathy and emotional responses. Repeated rejections, perceived “failings” on our part and collapsed relationships have taught us to hold it all inside whatever the cost. Lived experience tells us that we are not safe acting as ourselves in the world at this time. It can be hard to know where the line is between who we inherently are, and who we are pretending to be.We may know when we are okay to be around other people, scheduling our social engagements around our menstrual cycle. Some days and weeks we can’t be trusted to people.As highly sensitive people, we respond to our hormones with the entirety of our minds and bodies, and so we may avoid certain people and activities when hormonal volatility is predicted.Hormonal flux becomes unpredictable as we approach the menopause transition. We no longer possess the self-regulatory capacity to moderate our every word, action and facial response. Regressions in functioning occur, and our second nature skills of masking are lost. It can be terrifying to go into meltdowns from triggers that you have coped with masked for decades.In perimenopause, this can trigger the sense of intense loss of self.But there is light at the end of the tunnel. In the later stages of neurodivergent perimenopause and beyond, fewer f***s are given. Literally and metaphorically.We can come back to ourselves, find our neurotribe, and settle into a lifestyle that lends itself to managing our energy expenditure. We align the generous gift that is our empathy where it is validated, wanted and most needed.Neurodivergent-driven research on the topic of empathy in the menopasue transition is developing, and what follows is a selection of the work on empathy so far.The Double Empathy ProblemMany of us late diagnosed neurodivergent adults will have come across the theory of the double empathy problem whilst trying to figure out why we have felt so misunderstood for much of our lives. Often attributed as an issue for autistic people when communicating (or trying to) with neurotypicals, the double empathy problem originates from a much wider concept.First coined “the double empathy problem” by autistic researcher and sociologist Dr. Damian Milton in 2012, Milton drew on the notion that people of different cultures may often struggle to find some common ground, and experience communication breakdowns in the process.‘Simply put, the theory of the double empathy problem suggests that when people with very different experiences of the world interact with one another, they will struggle to empathise with each other. This is likely to be exacerbated through differences in language use and comprehension.’UK National Autistic Society: The double empathy problemMisunderstandings in mixed neurotype relationship dynamics have for too long been considered the fault of the neurodivergent partner. And this goes for all types of neurodivergence, despite the strong link the autistic community has with the double empathy problem. It is just as likely to be an issue for a stereotypically enthusiastic and energetic ADHDer or AuDHDer to be brushed off as “annoying” and “too much”.The double empathy problem theory provides reassurance that we are not the problem. Our supposed social deficits and communication differences are only apparent and obstructive when we are communicating with people who do not share our neurotype.This is why finding our neurotribe is invaluable to adults who self-identify as or are diagnosed neurodivergent. “I don’t understand you” is too frequently said to neurodivergents by their neurotypical partners, as though they are just not trying hard enough to make themselves understood. There is often very little flexibility from the neurotypical to try to understand their partner, who may already be struggling and exhausted from every single interaction, every single day.The time it takes for this awareness to occur can cost us our self-compassion, self-esteem and even our sense of self. Not wanting to face rejection after rejection, we learn from every social exchange with neurotypicals, and tweak our responses accordingly. It is not uncommon for later in life self-identified and diagnosed neurodivergents to have adopted another persona entirely.Masters of mimicry, and driven by a biological human instinct to be accepted, too many of us spent our formative years studying (and failing) how to appear acceptable, on the social periphery studying peers in the playground, obsessive book character analysis, copying soap opera stars’ mannerisms and so on.Hopefully our younger neurokin no longer need to do this because surely all the teachers, SENCOs, practitioners and parents are clued up about the double empathy problem by now..?The Triple Empathy ProblemHave you ever visited a healthcare practitioner and felt like you have not been understood, validated and treated appropriately?Unfortunately, this has been the norm for neurodivergent patients for all too long. Sometimes complicating factors make us seem too hard for the average doctor to want to work collaboratively with us. Finding healthcare providers who are willing to learn about nuances in health profiles, such as differing cultural and ethnic groups, co-occuring chronic health conditions, mental health conditions and increased likelihood of gender dysphoria and/or being trans can make medical visits feel harder than they need to be.On average, autistics and ADHDers have shorter life expectancy than neurotypicals. This may be because we do not experience pain and report symptoms in the manner medical professionals are used to. Sensory overload in clinical settings may reduce our capacity to engage. Executive functioning challenges make it a struggle to book and attend appointments, collect prescriptions, and remember to take our meds. There is a myriad of reasons why our life expectancy is shorter due to our neurodivergence, but it is unacceptable and shouldn’t be our burden to carry alone.Why is this not widely known, and managed as a systemic health crisis?In 2023, Shaw et al. took the double empathy problem theory, situated it within the medical context, and coined the term the triple empathy problem.‘Patients struggle to see their doctor’s perspective, and doctors can also struggle to see their patients’ perspectives. For example, when doctors are patients themselves, they experience healthcare with their own medical knowledge. The difficulty is seeing the perspective of a patient without any medical knowledge. Similarly, autistic people struggle to see non-autistic people’s perspectives and vice versa. So, it proves even harder for autistic patients to see their (non-autistic) doctor’s perspective, and even harder for (non-autistic) doctors to see autistic patients’ perspectives… This triple empathy problem may also be at play when autistic people interact with other professions and services, such as education, social care or the justice system.’Barriers to healthcare and a ‘triple empathy problem’ may lead to adverse outcomes for autistic adults: A qualitative study by Shaw et al. (2023)In my experience, working collaboratively on my medical issues has been best achieved when my healthcare providers are neurodivergent themselves. Unfortunately, it is not always safe for doctors and health practitioners to disclose their own neurodivergence in the workplace. Proactively seeking neuro-affirming medical staff throughout our lifespan to support us could be most effective, giving us the best possible health outcomes. Yet self-advocacy can still be extremely challenging, especially when we are already feeling depleted and sick.Training is essential for this travesty to be corrected, and there are recommendations for healthcare practitioners to adopt in order for our neurodivergent cultural differences in social communication, pain response and identification plus other variations to be best accommodated.Building on Shaw et al’s findings, Doherty et al. (2023) developed Autistic SPACE: a novel framework for meeting the needs of autistic people in healthcare settings.‘This (the Autistic SPACE framework) encompasses five core autistic needs: Sensory needs, Predictability, Acceptance, Communication and Empathy. Three additional domains are represented by physical space, processing space and emotional space. This simple yet memorable framework encompasses commonalities shared by autistic people.’Autistic SPACE: a novel framework for meeting the needs of autistic people in healthcare settings by Doherty et al. (2023)The Doherty et al. paper is packed full of great information on neurodivergent inclusivity that should be compulsory reading for all patients, medical staff, therapists, holistic practitioners and health boards. I strongly encourage you to take a look at the table of Recommendations for supporting Autistic SPACE in practice, because I think you will feel totally validated. (Screenshots of the table are below, with credit to Doherty et al., 2023).Sensory processing disorder is a form of neurodivergence that co-occurs extremely highly with autism and ADHD, and we all have differing sensory sensitivities and tolerance levels. Hormonal fluctuations during perimenopause and beyond exacerbate these differences, and can make day to day life feel torturous. Temperature dysregulation can worsen, joint pain may feel agonising, and menstrual cramps can combine, putting us into a sedentary lifestyle.Shutdowns, meltdowns and periods of inertia may increase, forcing our functioning to plummet to a debilitating extent.Spiralling hormones drive our mood, cognition and energy levels to spiral too. Just when we have the least capacity to understand what is going on for ourselves and self-advocate, we need to do so more than ever before.The Quadruple Empathy ProblemWidespread symptoms of the menopause transition may affect neurodivergent people to the extreme. The mind and body effects of fluctuating oestrogen, progesterone and testosterone production can lead to regressions and an inability to function. This was certainly the case for me, but I hope you are faring better!Midlife burnout for neurodivergent women and AFABs is often misattributed to factors other than hormonal flux, and therefore we are prone to being misdiagnosed and medical gaslit, resulting in inappropriate treatment.In their 2024 study “A perfect storm”: Autistic experiences of menopause and midlife, Brady et al. identified menopause as the fourth dimension of the empathy problem.Shaw et al. (2023) described a triple empathy problem where autistic people struggle to make themselves understood and understand those of other neurotypes in the context of medical settings.We found an added dimension where communication challenges were even more profound for some autistic participants transitioning through menopause, combined with what we would characterize as medical misogyny; this could be seen as creating a quadruple empathy problem.Some participants indicated that menopause was reminiscent of former experiences of hormonal transition like puberty and menarche, transitions in which they had also struggled with communication…… A key takeaway is the importance of person-centred, autism-informed healthcare that considers intersectionality and accessibility needs. We encourage healthcare professionals to recognize autistic communication styles and the various symptoms of menopause, including those that are less widely discussed, and to be receptive to the fact that menopause may start earlier than is commonly expected.Brady et al. (2024) “A perfect storm”: Autistic experiences of menopause and midlifeMedical gaslighting of neurodivergent menopause is still prevalent, with women and AFABs being told we are too young to be experiencing symptoms. When neither the practitioner nor the patient are well informed about menopause and/or neurodivergence, the chances of appropriately treating her symptoms are extremely unlikely.There is also some emerging research into ADHD and menopause, such as the academic paper ADHD in females: Survey findings on symptoms across hormonal life stages by Osianlis et al. (2026). Their results showed that 97.5% of participants perceived a worsening of ADHD symptoms during menopause, but as it was self-reported data, there are limitations in extrapolating these findings. However it does suggest that more research is needed in this area.As an AuDHDer, I find it concerning that research continues to polarise women and AFABs by their neurodevelopmental conditions. Surely we don’t need to continue studying ADHD and autism separately when both co-occur so strongly. I cannot separate the effects of menopause on my ADHD versus my autism as they are equally integral to my human experience.If widely applied in medical settings, the Autistic SPACE framework shared above could transform our interactions within the healthcare system, and improve our life chances.With so many multipliers to the empathy problem, neurotypical people need to take equal responsibility in understanding how neurodivergents perceive and cope in this world which rarely has our best interests at heart. Children should be accepted as they are, without having to waste their childhoods fawning “normal”, regardless of their neurotype.By the time the younger generation growing up today reach midlife, this all needs to be understood and standard practice within all healthcare institutions. Neurodivergent friendly medical settings and neuro-affirming practitioners will enhance our life chances, whilst providing the validation and supports we have lacked for so long.I would love to hear from you in the comments!* Do you relate more to the double, triple or quadruple empathy problem?* Do you feel the biggest empathy breakdowns happen in your relationships, healthcare, workplace or family?* Has your menopause transition affected your experience of giving and receiving empathy?Cheers,P.S. Please excuse typos and general nonsensical grammar. This essay taken me hours and hours and hours to write, edit, review, rewrite, edit, record the audio voiceover and upload to publish. Whilst I can report an astonishing improvement in my quality of life now that I am in surgical menopause, the lingering effects of the heavy sedation and general anaesthetic from August 2025 are still with me. 😵💫If this resonated, you are not alone — and you deserve spaces where your empathy isn’t pathologised. Paid subscribers help sustain this work and gain access to deeper dives, research breakdowns, and a community that empathises with you. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 25m 42s | ||||||
| 1/16/26 |  This Barbie Has No More F***s Left 💕 🌸 🎧 | For anyone who’s ever silently lost their s**t at doctors, hormones, or Ken: this is your AuDHD Barbie, finally done pretending. Originally titled. "Introducing AuDHD Barbie".Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer, and I have recently had a hysterectomy. As a neurodivergent perimenopause and PMDD survivor, I offer peer support and share knowledge on how to make it through the hard times.Thanks for joining me on this wild midlife ride! 🎢This is a snapshot in time of Barbie in midlife, who is late diagnosed Autistic, with co-occuring ADHD (AuDHD), in the throes of hormonal flux and she does not have enough f***s left to give.In this spoof piece, let me take you into Barbie’s messy Dream House where our protagonist can safely self-regulate and drop her social mask…AuDHD Barbie - or just “Barbie” to her friends - ignored her ringing phone, as Ken came through to her voicemail message: “Hi, it’s Barbie. Please do not leave a message. Text me, but only if it is important. Bye.”“For f**k’s sake, Ken”, Barbie muttered under her breath finally picking up as Ken rang through yet again. “This had better be important”, Barbie seethed down the line. “No, I don’t want to go to the beach party. I already told you! None of my clothes fit me anymore and my stupid period just started. How can I be bleeding again? It is only sixteen days since my last - hello? Ken?!”The dead phone line was the most soothing sound Barbie had heard all day.Barbie high fived herself. Period talk always made Ken cut his conversations short. Barbie believed that sand was cursed, and a cold shiver coursed through her body at the thought of ever having to go to another beach party again. This gave some light relief to her otherwise 24/7 hot flush. It was all right for Ken to go, he wasn’t experiencing hormonal mania making him rapidly lose muscle mass, bone density and his entire sense of self.Yes, things were just fine for Ken as always. Whilst he grinningly pumped iron and mainlined a creatine and protein powder blend on the daily, Barbie was forgetting to eat. Her only exercise was to burn calories through hanger-induced meltdowns. Her lifelong body dysmorphia was now at its peak.Looking down at her bloated meno belly, Barbie felt that she was retaining more water these days than there was in the entire ocean. ‘Calorie deficit diets’ were no longer working for her. Nor was intermittent fasting, the 5-2, Mediterranean, Paleo, Keto, Whole30, low FODMAP, low histamine, or eating only even numbered quantities of beige foods during even numbered hours of the day.Barbie collapsed into her sensory swing, kicked off her high heels and threw them across the room. They had been digging into her cankles, and she applied an ice pack to the ankle she had badly rolled earlier that day. Not for the first time, she dry heaved at the sight of the thick dark hairs growing at right angles out of her once dainty feet and toes.What is wrong with me? she wondered to herself. I used to love beach parties and hanging out with Ken. Now I just want to kill him every time he comes near me! God, he is such a dick.Barbie excavated the teetering mountain of hot pink dirty laundry to find the remote control for her cooling fan, trying not to disturb her sleeping cats. Turning her fan on to the max helped redistribute the air flow, which was currently carrying the unmistakable odour of the cat s**t in the nearby litter box.For f**k’s sake, Ken! Barbie thought to herself again, as rage filled every fibre of her being faster than any number of mindful deep breaths could diffuse. Scooping the cats’ s**t is a blue job. Why haven’t you f*****g done it?Even if she had wanted to, Barbie couldn’t scoop the litter boxes; not with her tennis elbow, frozen shoulder and splinted hypermobile wrist that her doctor had said in no uncertain terms were not symptoms of perimenopause.“Well, Ms AuDHD Barbie, you are in the prime of your life”, the doctor had told her earlier that day, whilst attempting to look both up her itchy short skirt and down her scratchy scoop neck top. Barbie could feel hives emerging across her chest, but she resisted agitating them with her brittle nails. She would wait until she got home, and then rub them raw until they bled. Bliss!“Allow me to assure you that you are too young to be experiencing menopause symptoms”, her doctor went on. “And, might I add, that you do not look autistic, and you are far too successful to have ADHD. Your lab results are fine. Your estradiol is at normal levels. You are still a very fertile young woman.”His lack of eye contact was now vexing her, ironic given that her own reported discomfort at holding a gaze was flagged in her recent autism assessment. Yes, for decades she had masked endlessly, with her iconic plastic moulded smile rouged to constant perfection. But now she felt ready to tear off the mask and stamp on it right there and then in the doctor’s office.“Look,” the doctor had gone on, “I will note your concerns but, for the record, I am of the professional opinion that you have nothing at all to worry about. You are seeking diagnoses unnecessarily. There is no cure nor treatment for neurodivergence or perimenopause anyway. This trend of over diagnosing autism and ADHD is getting out of hand! We all know that males are 1,000,000 times more likely to be neurodivergent than females. Not to mention the fact that women cope with it. Why would a woman of your standing want a diagnosis when you have managed fine all your life until now?”Barbie was mute. Situationally, not selectively. Despite scripting the discussion in advance over and over in her head, she could feel her neck and face burning, hot tears pricked her eyes. She sniffed them back. A thousand retorts would fire around her mind like pinballs in the hours and days that would follow, yet for now she froze in despair and panic. Her ever saggier face remained static, fixed with a wry smile. Barbie’s now unfocused eyes were blurring off into the distance, as she wished she could be anywhere else.“This is all in your pretty little head. How does Ken feel about all of this?”, the doctor went on. “I can increase your SSRI dose but I cannot offer you hormonal therapy because the significant risks are not worth the supposed benefits. You are fine. Keep doing what you are doing. I am here any time you need to see me for support and advice.”Barbie was already so f*****g sick of being objectified and patronised, but medical gaslighting was a new one on her. She decided not to tell this professional pervert all the other worries she had noted down to prompt the consultation. Bleeding gums. Loose teeth. Itchy ears. Cognitive decline. Urinary incontinence. Insomnia. Losing all her stuff. Suicidal thoughts. And that the sight of Ken in all his so-called glory did nothing for her anymore, and that she was feeling dead inside. Particularly ‘downstairs’. Her vagina was rapidly becoming nothing short of warped, and some prolific Googling of the mind-blowing symptoms of perimenopause had led to a self-diagnoses of vaginal atrophy and pelvic organ prolapse.If Ken only knew that my vag feels like someone has taken a cheese grater to it, and that my kamikaze uterus is doing it’s best to sacrifice itself, Barbie thought, he might stop calling me all the time and let me live in peace.No. Despite feeling broken, Barbie hadn’t mentioned her more sensitive gynaecological ailments to this doctor, and instead made a mental note to find a neuro-affirming menopause specialist doctor, and develop her self-advocacy skills.Back in the sensory sanctuary of her Dream House, Barbie slipped into something a little more comfortable to see her through her impending shutdown. A black hoodie, compression tights that covered her multitude of coffee table bruises, and her noise cancelling earbuds. She zoned out listening to a perimenopause podcast to help her feel sane, informed and less alone.Barbie took off her shiny sleek blonde wig to free her own matted, unwashed hair, doused her hair in dry shampoo then tied it back out of her face. The regular intrusive thought of shaving her head returned, and she blinked and cleared her throat ten times whilst humming to try to make it stop, whilst pulling out tangled clumps of fallen hair from between her fingers. Barbie was alarmed at the amount of hair she was losing, and her male pattern hair loss and receding hair line made her cry in secret most days. The wig was just easier now than dealing with her own hair, and facing questions about it.Until she found a better doctor, she didn’t have the right answers anyway.🩷 How are you feeling about Mattel’s announcement of the new Autistic Barbie? 🩷Let me know in the comments!Cheers,andThanks for reading Divergent Menopause. Paid subscribers make this work possible. 💕🐈 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 10m 52s | ||||||
| 1/3/26 |  (Live) Perimenopause, Medical Gaslighting and Estrogen Patch Inefficacy | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I’m Sam Galloway (she/her) and I am an AuDHD woman four months into surgical menopause (hysterectomy and oopherectomy).If you are interested about why I needed the surgery, you can read more here.Thanks for joining me on this wild midlife ride! 🎢Thank you to everyone who tuned into my live video with Sonia Voldseth, the creator of Menopause & Misogyny! TL;DR * This advocacy-focused conversation documents real harm caused by estrogen patch failures and loss of choice in Aotearoa New Zealand. * When menopausal and neurodivergent women aren’t believed, symptoms escalate into cognitive, emotional, and physical crises. * Menopause care is essential healthcare. It is not optional, not cosmetic, and not something women should have to fight this hard to access.Sonia and I are both fortunate enough to live in Aotearoa New Zealand. Sonia, originally from the United States, lives surrounded by mountains in Queenstown on the South Island, and I, London Irish in origin, enjoy beachside life on the Kāpiti Coast near the bottom of the North Island.Unfortunately Sonia and I have both been affected by the ongoing oestrogen patch debacle. In 2024, we saw a global shortage of oestrogen patches, which I wrote about here. Currently there is laboratory testing underway in response to many people reporting that their menopause symptoms have returned despite staying on the same dose and brand. This has coincided with a new formulation of this vital hormone therapy treatment. My fellow pedants may notice that today I can’t decide whether to spell it “oestrogen” (UK and NZ) or “estrogen” (US), but please know that I am referring to the same hormone, regardless of the spelling used.Remarkably, the sedatives and general anaesthetic still have lasting effects on my capacity to write articulately, now four months after my total hysterectomy with bilateral salpingo oopherectomy (cervix, uterus, ovaries and Fallopian tubes removed). Surgical menopause has been life saving to my mental health, energy capacity and general functioning, so I am not complaining. But, rather than feeling able to summarise our discussion myself, instead I include ChatGPT’s offering below.As ever, for accessibility, you have the options to watch the video (with or without closed captions), listen to the audio and/or read the transcript. AI-Generated Timestamped Summary00:00 — Why this conversation matters02:31 — Progress made… then undone05:31 — Estrogen patch shortages & loss of choice (NZ)09:01 — Symptoms returning on the same dose12:01 — Collective patterns, individual gaslighting15:31 — Neurodivergent risk & mental health impacts18:31 — Estrogen as a brain hormone22:01 — Why “just switch to gel” isn’t simple25:31 — Sleep collapse as the red flag28:31 — Admin, advocacy & exhaustion32:57 — Suspected formulation change (mid-2025)34:31 — Medsafe reporting & deflection36:05 — User-error narratives & systemic gaslighting37:42 — Absorption differences & dosing reality39:58 — Brain fog, language loss & regression41:25 — Estrogen receptor saturation explained44:19 — Menopause is serious, not “just hot flushes”45:37 — Generational harm & WHI fallout47:03 — Surgical menopause & compounded harm48:37 — Aging with quality of life49:30 — Vaginal estrogen, bladder health & prolapse prevention52:35 — Prolapse, gatekeeping & specialist care54:38 — Medical training gaps (global)55:10 — Vaginal estrogen & cancer-risk reassurance56:07 — Solidarity over infighting56:56 — Closing reflections, access & hopeThank you to fellow AuDHDer and PMDD survivor Kim Pitts for chatting with us in the comments about her personal experience of menopause and medical misogyny. Kim and I have previously chatted live (link below) and here is Kim’s Auti Peri Q&A.Cheers,SamThis work exists through collective care. A paid subscription is a meaningful way to support Divergent Menopause in 2026. Thank you! 💕 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 1h 01m 00s | ||||||
| 1/2/26 |  Anti-Goals: When Goal-Setting Makes Things Worse | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I’m Sam Galloway (she/her) and I am an AuDHD woman four months into surgical menopause (hysterectomy and oopherectomy).If you are interested about why I needed the surgery, you can read more here.Thanks for joining me on this wild midlife ride! 🎢Hello and Happy New Year to you!And just like that we are in 2026. Hooray, we made it! Ageing is a privilege, but it isn’t easy. All we can do some days is take one step at a time, one breath at a time, and keep on keeping on. And that is more than enough. Around this time last year I wrote an article about Anti-Goals, and it is still being read and shared daily! It is by far my most popular post so far, and it captures the spirit of those of us who reject and repel the January conventions of self-improvement.Demand avoidance is running high in my life and I have long been wanting to write a follow up article. My brain has forbidden it though, so I have compromised with myself and recorded this follow up video on the topic for now instead. As always, the video is optional and is accompanied by an audio only podcast alternative, and/or a transcript. For accessibility’s sake, I also include below a timestamped summary provided by ChatGPT. What’s helping you get through right now?What do you wish you had more support with?If you want to share in the comments, you’re welcome to.One word or an emoji is more than enough.⏱️ AI-Generated Timestamped Breakdown00:00 – New Year’s resolutions are nonsense (for many of us)Why January pressure is unrealistic, especially during hormonal flux, and why time is a social construct anyway.00:01 – Why goal-setting can fail demand-avoidant brainsIntroducing anti-goals and why avoiding harm can be more useful than striving for achievement.00:02 – When survival becomes the goalWhat anti-goals looked like at my lowest point: reducing pain, anxiety, depression, and suicidal ideation.00:03 – You can’t reverse a spiral aloneWhy support and a plan matter — and why “starting from scratch” isn’t possible when you’re already overwhelmed.00:04 – Different baselines, different needsWhy comparing yourself to people “optimising” their lives is harmful when you’re just trying to get through the day.00:05 – Redefining success at homeFrom magazine-perfect homes to hygienic and safe: using tools (like a robot vacuum) to reduce energy drain.00:06 – Pain management over fitness goalsWhy “I don’t want to be in pain” is a valid goal — and how medical support, warmth, medication, and pacing mattered more than exercise plans.00:08 – Addressing the root causeHow hormonal instability drove pain, mood changes, and loss of self-care capacity — and why treating that came first.00:09 – Hormonal treatment and surgeryMy path through HRT, chemical menopause, and ultimately hysterectomy/oophorectomy — and how stability changed everything.00:11 – Survival before self-improvementWhy health span matters more than optimisation, and why there is still no clear medical model for neurodivergent menopause.00:12 – Don’t waste energy on unachievable goalsChoosing meds, blood tests, and basic care over gyms, meal prep, or “doing it properly”.00:14 – Accepting support is not failureWhy masking through struggle is dangerous — and how getting help allows us to later help others.00:15 – Hormones as a buffer, not a cureMedication, therapy, cleaners, junk food, respite — whatever helps you get through now is valid.00:16 – Incremental change, not January transformationsWhy progress is slow, nonlinear, and includes regression — and why that’s not shameful.00:18 – Spending energy and money wiselyLooking at root-cause support (pelvic physio, hormone care, surgery pathways) rather than short-term coping fixes.00:19 – What do you need right now?An invitation to reflect, share in the comments, and focus on getting through 2026 and beyond.💛 Key TakeawayIf you are neurodivergent and navigating perimenopause or menopause, your job is not to optimise yourself.Your job is to stay alive, reduce suffering, and be kind to yourself while you transition through this phase.Everything else can wait.That’s all for now. It is bedtime here and I am delighted to report that my menopausal sleep is phenomenally better than my perimenopausal sleep was this time last year! I hope that whatever you have planned for today, that you can afford yourself some peaceful time to rest. Cheers,SamIf this post helped you feel a little less alone, a paid subscription is how you support this work and help keep it going. No pressure! Just here if and when it feels right. 😊 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 19m 48s | ||||||
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 11/25/25 |  🎧 4: Can your creativity change as you change? | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer, and I have recently had a hysterectomy. As a neurodivergent perimenopause and PMDD survivor, I offer peer support and share knowledge on how to make it through the hard times.Thanks for joining me on this wild midlife ride! 🎢I am delighted to be joined again by Allegra Chapman (she/her) from Creative Fix in the final episode of Divergent Creativity in Menopause!Together Allegra and I have created this four part mini series on the importance of creativity during the menopause transition and beyond. 🎧 1) What is creativity is and why does it matter?🎧 2) How can creativity fit your needs?🎧 3) Can you be creative by accident?🎧 4) Can your creativity change as you change?In this fourth and final part we talked about: 💕 Creativity shifts as our needs change throughout fluctuating capacity in neurodivergent perimenopause and beyond. Our creative practices can adapt and may become slower, smaller, or look entirely different.💕 Creativity is a tool for unmasking and self-understanding. It helps us process our emotions (even when alexithymia makes them hard to name), recognise our needs, and navigate a world not built for neurodivergent, disabled or midlife women.💕 There is no “right way” to be creative. We don’t need to follow neurotypical or traditionally masculine productivity advice. Creativity can look like writing novels or doodling, resting, or simply daydreaming. Whatever works for you is the right way. Writing an autism adapted suicide safety planis creative because you’re thinking about what are your triggers,what do you need, and what needs to be on hand. And then also about havinga toolkit you know to keep you regulated, regulate your nervoussystem and then that that’s also creative to meet your needs. You don’t alwayshave to be doing something.Sam Galloway Further reading and resourcesAllegra’s inspiring book ‘Creativity is your self-care: 52 creative therapy exercises exercises to support your emotional wellbeing all year round’ is available to buy here!If you would like to immerse deeper into Allegra’s creative wisdom, you can sign up to her course, Divergent Creatives.The online programme to enable neurodivergent or disabled people to build a sustainable and joyful creative practice. If you’re a writer or artist who has more ideas than you know what to do with, but you struggle to finish things, or even to get started, then this course is going to help you get sh*t done!A group of autistic menopause researchers based in the UK and Canada invited creative submissions reflecting people’s lived experience of this often challenging life transition. They wrote a paper on the submissions called ‘Stepping into who I fully am: A creative exploration of Autistic menopause.’Creative exploration of Autistic menopause encouraged emotional catharsis, self-understanding, and activism/artivism. Autistic Community Researchers noted transcendent, almost “magical” dimensions of connecting with other Autistic people’s lived experiences. Our creative emancipatory approach enabled Autistic, multimedia responses which traditional research methods would not have elicited…… Traditional research methods have limitations in capturing lived experiences of the Autistic menopausal transition. In this study creative, multimodal, arts-based approaches enhanced understanding by capturing nuanced interpretations and meanings.The ability to communicate through creative submissions facilitated participants’ self-expression and they recognised the potential therapeutic value of the creative process, as a “remedy” for Autistic menopause related difficulties.This study adopted a novel approach to data analysis in which Autistic community researchers used creative, reflexive approaches to respond to arts-based submissions rather than relying on traditional academic methods.For both Autistic research participants and Autistic researchers, creative methods had the potential to act as a catalyst for activism, artivism, and self-actualisation, encouraging personal transformation and magical transcendence through a process of (to paraphrase one of our participants) “stepping into” who we fully are.Stepping into Who I Fully Am: A Creative Exploration of Autistic MenopauseAuthor(s): Mx Rose Matthews , Christine A. Jenkins , Margaret Janse van Rensburg, Miranda J. Brady, Rachel L. Moseley, Julie M. Gamble-TurnerPublication date (Electronic, pub): 27 June 2025This concludes our series, and we hope you have enjoyed it! Thanks so much again to Allegra for recording this great chat with me, and thanks also to you for reading and listening! Cheers,If Divergent Menopause has helped you feel seen, understood, or a little less alone, please consider becoming a paid subscriber. Your support helps me keep this space accessible, and funds time to create more honest writing, Q&As, and resources for our neurodivergent menopause community. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 21m 26s | ||||||
| 11/18/25 |  🎧 3: Can you be creative by accident? | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer, and I have recently had a hysterectomy. As a neurodivergent perimenopause and PMDD survivor, I offer peer support and share knowledge on how to make it through the hard times.Thanks for joining me on this wild midlife ride! 🎢I am delighted to be joined again by Allegra Chapman (she/her) from Creative Fix in the third episode of Divergent Creativity in Menopause!Together Allegra and I have created this four part mini series on the importance of creativity during the menopause transition and beyond. 🎧 1) What is creativity is and why does it matter?🎧 2) How can creativity fit your needs?🎧 3) Can you be creative by accident?🎧 4) Can your creativity change as you change?In this third part we talked about: 💕 Taking natural seasonal items home to curate our own arrangements.💕 Finding beauty in dried flowers over fresh flowers these days as my skin and body become increasingly dry in menopause!💕 Noting down your accidental creativity using the downloadable sheet in this post from Allegra. It’s time to reclaim your creative nature and take note of just how much creativity you bring to the world without even realising it. Then, hopefully, you can give yourself permission to explore your creativity further, with more intention, and see where else it wants to take you!Allegra ChapmanWhat natural treasures can you find where you live?🍁🐚🌸Further reading and resourcesAllegra’s inspiring book ‘Creativity is your self-care: 52 creative therapy exercises exercises to support your emotional wellbeing all year round’ is available to buy here!If you would like to immerse deeper into Allegra’s creative wisdom, you can sign up to her course, Divergent Creatives.The online programme to enable neurodivergent or disabled people to build a sustainable and joyful creative practice. If you’re a writer or artist who has more ideas than you know what to do with, but you struggle to finish things, or even to get started, then this course is going to help you get sh*t done!A group of autistic menopause researchers based in the UK and Canada invited creative submissions reflecting people’s lived experience of this often challenging life transition. They wrote a paper on the submissions called ‘Stepping into who I fully am: A creative exploration of Autistic menopause.’Creative exploration of Autistic menopause encouraged emotional catharsis, self-understanding, and activism/artivism. Autistic Community Researchers noted transcendent, almost “magical” dimensions of connecting with other Autistic people’s lived experiences. Our creative emancipatory approach enabled Autistic, multimedia responses which traditional research methods would not have elicited…… Traditional research methods have limitations in capturing lived experiences of the Autistic menopausal transition. In this study creative, multimodal, arts-based approaches enhanced understanding by capturing nuanced interpretations and meanings.The ability to communicate through creative submissions facilitated participants’ self-expression and they recognised the potential therapeutic value of the creative process, as a “remedy” for Autistic menopause related difficulties.This study adopted a novel approach to data analysis in which Autistic community researchers used creative, reflexive approaches to respond to arts-based submissions rather than relying on traditional academic methods.For both Autistic research participants and Autistic researchers, creative methods had the potential to act as a catalyst for activism, artivism, and self-actualisation, encouraging personal transformation and magical transcendence through a process of (to paraphrase one of our participants) “stepping into” who we fully are.Stepping into Who I Fully Am: A Creative Exploration of Autistic MenopauseAuthor(s): Mx Rose Matthews , Christine A. Jenkins , Margaret Janse van Rensburg, Miranda J. Brady, Rachel L. Moseley, Julie M. Gamble-TurnerPublication date (Electronic, pub): 27 June 2025Next week Allegra and I will be sharing the fourth and final part of our podcast mini series with you. Have a great week!Cheers,Enjoying Divergent Menopause? Become a paid subscriber to support independent writing on neurodivergent midlife and menopause. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 11m 31s | ||||||
| 11/10/25 |  🎧 2: How can creativity fit your needs? | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her), an autistic ADHDer, and I have recently had a hysterectomy. As a neurodivergent perimenopause and PMDD survivor, I offer peer support and share knowledge on how to make it through the hard times.Thanks for joining me on this wild midlife ride! 🎢“Care for your needs as a priority, rather than leaving them at the bottom of the list.”I am delighted to be joined again by Allegra Chapman (she/her) from Creative Fix in the second episode of Divergent Creativity in Menopause!Together Allegra and I have created this four part mini series on the importance of creativity during the menopause transition and beyond. 🎧 1) What is creativity is and why does it matter?🎧 2) How can creativity fit your needs?🎧 3) Can you be creative by accident?🎧 4) Can your creativity change as you change?In this second part we talked about: 💕 how societal expectations and internalised ableism combine to make us de-prioritise our creativity💕 giving ourselves permission to meet our needs, and pacing our creative endeavours around our menstrual cycles/menopause stage 💕 being unable to do our best creative work if we are in neurodivergent burnout.Everyday creativity can be free, low key and take place both in the home and out and about.Resources and further readingAllegra’s inspiring book ‘Creativity is your self-care: 52 creative therapy exercises exercises to support your emotional wellbeing all year round’ is available to buy here!If you would like to immerse deeper into Allegra’s creative wisdom, you can sign up to her course, Divergent CreativesThe online programme to enable neurodivergent or disabled people to build a sustainable and joyful creative practice. If you’re a writer or artist who has more ideas than you know what to do with, but you struggle to finish things, or even to get started, then this course is going to help you get sh*t done!Dr Samantha Newman AKA Female GP Monthly Cycling “Your menstrual cycle is a natural process made up of four key stages: Menstruation, Follicular, Ovulation, and Luteal. Knowing how these stages work helps you better understand your body and mind.”Kate Codrington Menopause facilitator, speaker and author (Moon and Menopause tracking)Red School Menstrual cycle and menopause awarenessA group of autistic menopause researchers based in the UK and Canada invited creative submissions reflecting people’s lived experience of this often challenging life transition. They wrote a paper on the submissions called ‘Stepping into who I fully am: A creative exploration of Autistic menopause.’Creative exploration of Autistic menopause encouraged emotional catharsis, self-understanding, and activism/artivism. Autistic Community Researchers noted transcendent, almost “magical” dimensions of connecting with other Autistic people’s lived experiences. Our creative emancipatory approach enabled Autistic, multimedia responses which traditional research methods would not have elicited…… Traditional research methods have limitations in capturing lived experiences of the Autistic menopausal transition. In this study creative, multimodal, arts-based approaches enhanced understanding by capturing nuanced interpretations and meanings.The ability to communicate through creative submissions facilitated participants’ self-expression and they recognised the potential therapeutic value of the creative process, as a “remedy” for Autistic menopause related difficulties.This study adopted a novel approach to data analysis in which Autistic community researchers used creative, reflexive approaches to respond to arts-based submissions rather than relying on traditional academic methods.For both Autistic research participants and Autistic researchers, creative methods had the potential to act as a catalyst for activism, artivism, and self-actualisation, encouraging personal transformation and magical transcendence through a process of (to paraphrase one of our participants) “stepping into” who we fully are.Stepping into Who I Fully Am: A Creative Exploration of Autistic MenopauseAuthor(s): Mx Rose Matthews , Christine A. Jenkins , Margaret Janse van Rensburg, Miranda J. Brady , Rachel L. Moseley , Julie M. Gamble-TurnerPublication date (Electronic, pub): 27 June 2025It is a pleasure to continue sharing my conversation with Allegra with you. I hope you are enjoying it, and that you are able to fit some crucial creativity around your current needs and within your fluctuating capacity. Cheers,If you enjoy these posts and want to fuel more of them, think of a paid subscription like buying me a coffee each month. It’s a small gesture that makes a big difference to keeping Divergent Menopause going strong. Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 12m 54s | ||||||
| 11/5/25 |  ADHD Meets Menopause: A Volatile Mix | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I’m Sam Galloway (she/her) and I am an AuDHD woman ten weeks into surgical menopause (hysterectomy).If you are interested about why I needed the surgery, you can read more here.Thanks for joining me on this wild midlife ride! 🎢October was World ADHD Awareness Month and World Menopause Awareness MonthAs you are here, chances are that you are already aware of both Attention Deficit Hyperactivity Disorder (ADHD) and menopause. I wish I had known about them sooner… but better late than never. We still don’t know enough about how the two intersect, but early research suggests that hormonal flux in neurodivergent brains and bodies may be suboptimal for our mental and physical health. To say that perimenopause sent me absolutely batshit cray cray would be a gross understatement. Why is awareness still the goal in 2025? Acceptance and gold standards of care should be where we are already at. Yet awareness it must be, since many of us have friends, family members and even healthcare teams who are not yet aware of the potential for volatility during the neurodivergent menopause transition. Why is ADHD affected by hormonal flux? Well, we don’t know yet. But Behrman and Crockett explain in their 2024 research paper, Severe mental illness and the perimenopause, that:Executive dysfunction and other cognitive problems are commonly reported during the perimenopause; these which can appear very similar to the constellation of symptoms seen in attention-deficit hyperactivity disorder (ADHD)32 and, like ADHD, can respond to stimulants.33 It is unclear whether this is an unmasking of underlying pre-existing ADHD or entirely de novo symptoms. Given the overlap, it can be hypothesised that those with pre-existing ADHD may experience a worsening of their ADHD symptoms with perimenopause, and it has been shown that people with comorbid ADHD are also more vulnerable to perimenopause-associated psychological symptoms.34There is much hypothesising in the field, whilst those of us deep in the trenches are falling daily on the battlefield. We may not know why menopause is such a challenging transition for many neurodivergent people, but we need to be alert to the risks. This is not a “Yay for ADHD !” article. Yes, there are advantages to having this condition, as there are also disadvantages. My ADHD wasn’t diagnosed until I was 39 - two years after my later in life autism diagnosis. I thought naively that by 40 I had all the answers, and would be able to live my best years going forward. I could not have been more wrong!I was only too glad to finally be aware of my neurotype, yet awareness is only the beginning. Forty five minutes into my hour long Zoom consult with an Auckland-based psychiatrist, my ADHD assessment was over and it was a done deal. He diagnosed me with ADD (which is an out of date diagnosis now, but whatevs). He hung up and spent the remainder of my allocated session writing up notes for my diagnostic report and filing the pharmaceutical admin to process the special authority number required for me to trial controlled stimulant drugs. Meanwhile, I sat alone in floods of tears weeping for Little Sam who had never stood a chance. Tears are welling up now (or trying to) in my menopausally dry eyes just from thinking back on it.As an AuDHDer (autistic and ADHD), I have learnt the long and hard way that the impact ADHD can have on our menopause transition can be catastrophic, isolating and feel deeply shameful.1 in 4 ADHD women have attempted suicide. Things are already hard for us during times of hormonal flux but we often make exceptions for people’s hormonal changes in puberty, pregnancy, postpartum and during menstrual periods and premenstrual dysphoria disorder (PMDD). Menopausal people also need accommodations and support. Knowing what to expect is crucial in then dealing with it. You aren’t broken and you don’t need to be fixed. You are enough and not too much. You deserve acceptance not awareness.To save you the time and energy on obsessively compulsively meticulously researching characteristics of adult ADHD, and the implications perimenopause has on ADHD, I am here to share the low highlights in no particular order:* It’s not called ADD (attention deficit disorder) anymore. ADD is no longer diagnosable. There are three types of ADHD: hyperactive, inattentive, and combined type. Combined means you are both hyperactive and inattentive.* Lagging skills versus inability. Neurodevelopment is slower for us. Immature behaviour and executive dysfunction do not determine intellect, regardless of our age. Remember that you have strengths. Play to them when and where you can. * You might see ADHD in your kids - especially boys - first, because their external hyperactive symptoms can manifest as “disruptive” in the classroom, and the teachers want to shut them down support them. * Your energy is exceptional and feels abundant, but you can crash hormonally. We can’t run on empty. Those of us who are exceptionally sensitive to hormonal flux will know all too well that we have had “good weeks” and “bad weeks” in our menstruating years. When those changes are catastrophic, it may indicate that we have premenstrual dysphoria disorder (PMDD). Previous patterns of mental health implications caused hormonally such as during menses, menstruation, pregnancy, postpartum, during IVF treatment etc. are indicators of future challenges during perimenopause. * Hyperactivity can be cerebral, not always physical. Overthinking, anxiety, rumination, sleep issues, scripting phone calls, imagining other worlds and embarking on new and illicit relationships in your head are allways it can manifest. We create these elaborate situations in our minds because our physical surroundings are understimulating or triggering. What’s more interesting than deciding what to cook for dinner yet again? Alternative lives, sliding doors, reimagined reality. When we are externally presenting as inattentive often it’s accompanied by internal hyperactivity which means that we are often combined type, even when diagnosed ADD, as I was. * Inattentiveness can be painful and shameful. We aren’t mishearing and daydreaming on purpose to annoy others - although they rarely see it that way. Part of the assessment process for ADHD includes presenting our old school reports to inform the diagnostic process. Proof that we have always been considered not good enough. Annually and without fail my end of year reports read, “Must try harder. Could do better. Not reaching potential.” Yet nobody in a classroom is trying as hard as a girl/AFAB who is endlessly having to suppress her rich and stimulating inner world and pass for normal.* People will tell you you’re wrong about ADHD, especially those with the least amount of experience or knowledge about it. They won’t want you to talk about it with them so, unless it is imperative to the safety of yourself or someone else, don’t waste your finite energy. Find your neurotribe, because they may want to talk about nothing else, and we can all geek out together on the wonders of being neuromagnificent! ⭐️* We see ADHD in others, usually long before they wish to accept it. They refuse the label, as if you are branding them like cattle, or trying to insult them. Bide your time, realisations can take a while and denial is real. Try to protect your own rejection sensitivity dysphoria (RSD) being triggered when they seem supportive of you being ADHD, yet when it comes to their own identity they are appalled at the suggestion. * RSD is painful and overwhelming. Rejection sensitivity occurs when we have been rejected, insulted, gaslit, dismissed or any manor of things by someone, whether they did so intentionally or not. We can really stew on it, and then be consumed by it. It feeds our negativity bias and need for cerebral stimulation until we have broken ourselves. I have found the best way to manage this is to recognise it, and stop myself from spiralling. Do what you can to stop building on the idea that you have been slighted. Even if they meant to upset you, screw them. Instead you can: stim, listen to a favourite song that uplifts you and takes you to another time or place, journal it then burn the page, get outside. As I was writing this around Halloween, you may also like to curse them and/or make a voodoo doll and inflict pain on them. Whatever you do, keep it short then move on. If it comes up in your head again, tell yourself you have already dealt with it, and that it is just the hungry RSD looking for your attention. * Boredom is our kryptonite and our brains will do anything to avoid it.* Hyperfocus can be productive or not, and it is hard to channel it. Unless it is harming someone, once you get into flow, lean into it. Hyperfocus is a beautiful process and don’t feel bad if you don’t end up with a completed project at the end. Just go to the toilet, drink some water and have something to eat, because you are likely to have forgotten that the concept of time exists, and that you live in human bodily form. * So-called hard things are easy for us: entrepreneurship; picking up and dropping new hobbies and interests as though our lives depend on it; changing careers; earning multiple degrees; pulling all nighters; spotting neurodivergence in others. These are not superpowers though, and we should not be made to excel beyond our capacity to meet other people’s expectations. Exploiting neurodivergent people’s strengths whilst ignoring our struggles puts us at risk of burnout and abuse.* So-called easy things are hard for us: sensing the passage of time, and thus punctuality; booking appointments; small talk; meal planning; remembering to take the meds that help us do all of the above. Basically anything requiring executive functioning can become increasingly difficult in perimenopause, not helped by increasing midlife demands of parenting, caring for ageing parents, managing a household, employment and so on. * Now/not now. Having no sense of time is a common issue. Rather than feeling time pass, I know I either need to do the thing in my calendar now or not now. Dopamine elicited from extreme time pressure is a huge motivator for me, which is why I am finally finishing this article that I intended to publish “for the start of October” a week into November. Time is but a social construct. Again: better late than never…* Dopamine isn’t always scrolling. Impulsivity means we often get caught speeding or we may overspend (I did both cyclically throughout my twenties). Not thinking through the longer term consequences of our actions is pretty common. When things feel bad, it feels like they’ll never change. Is this why our suicide rate is so high? 1 in 4 women have attempted suicide, and I worry that this is too often down to extreme impulsivity driven by hormonal flux.* Hormonal flux can drive us downhill rapidly, so be prepared. Some people are sensitive to changing hormone levels - the ups and downs - rather than the levels themselves. Prior to my chemical menopause and now my surgical menopause, my mood, executive functioning and capacity dropped faster than I could sense any internal changes. Rage would escape me unprovoked. Masking was impossible. I couldn’t recognise who I was any more in those moments and within a few short years I had become a husk of my former self.* ADHDers are rescuers. We can also be naive, easily taking advantage of, trusting and gullible. As change makers and trailblazers, we think we can change others too. We may hone in on a wrong’un and believe we are able to save them from themselves. Sometimes this can end up with us becoming abused, bankrupt and at risk. * A special interest/hyperfocus can be a person. We can be obsessed for an unknown length of time and all in our head, until it burns out and we are no longer interested. We may then never talk or think about that person ever again.* Object permanence. We aren’t vindictively ignoring loved ones, but out of sight means out of mind. We can forget people we have known for years even exist. That upsets us as much as it upsets them. If only we had the executive functioning to print, frame and hang photos, seeing their faces might jog our memory…* Can OCD (obsessive compulsive disorder) mask ADHD? Does hyperactivity plus productivity equal OCD? I’m jealous of ADHDers who also have just enough OCD to keep everything clean and tidy and be consistent. Without that I live in clutter, hoarding and tripping over my own stuff, yet remain unmotivated and disinterested in picking it all up. Add in two neurodivergent kids who take after me, and it’s a wonder we can walk around our home at all! Goblin mode is real. It’s not laziness, it’s different priorities, lagging executive functioning skills and an inability to motivate and mobilise myself. Stimulant medication helps with all of that to some degree, in my case.* We can be introverted or extroverted, and we will often appear to oscillate between the two. How much of this is masking versus exhaustion? ADHD can be an energy mismatch. Imagine yourself entertaining and running around at home looking after everybody (unless you get hit by a car and get to spend Christmas with your feet up, as I did last year), then you’re exhausted when everyone wants to go out and they wonder why you don’t want to go. You have enabled everyone else to rest, chat and chill whilst you have burnt yourself out. Just say you have a migraine and wave them off at the door. Surely you are due a good solo doom scrolling session now to re-boot? Enjoy!* When we can make it out of the house, we are first to read the room. We are instinctive and perceptive about events and behaviours before anyone else feels it. We may want to leave before everyone else does when things feel too intense. In our youth, and even into midlife, we might stay out and self-medicate with booze, drugs and/or chocolate fountains to dampen the sensory overload and stress. These are understandable ways of masking and self-soothing, but can be hard habits to break long after they stop serving us. If they ever did.* Sensory processing disorder (SPD) co-occurs strongly with ADHD, autism and other forms of neurodivergence. This can be tricky to self-identify because we mask so strongly and have decades of unlearning uncomfortable compensatory habits. Sensory seeking and sensory avoiding shapes our world view and capacity to go out into an uncontrollable world. Squinting in bright rooms because we were told wearing sunglasses indoors made us weird, and getting told squinting is weird, and no it’s not too bright. Sticking our fingers in our ears during fireworks displays, being scared of balloons popping at parties and dogs barking (just me?). Swigging cod liver oil from the bottle in my Nan’s cupboard because I sought out strong flavours. You know, normal stuff. 👀Do yourself a favour and read up on sensory processing difficulties and challenges, which includes interoception and proprioception (see below). If it is accessible to you, work with a neuro-affirming occupational therapist to create a personalised sensory diet, where you include movement snacks and tools such as weighted blankets, safe foods, noise cancelling headphones etc. on hand to regulate your sensory inputs. If it is inaccessible to you, then take a look on YouTube for ideas. * Interoception refers to interpreting our inner states such as hunger, thirst, pain etc. Some of us have heightened interoception and may feel pain to an extreme, whereas someone with a reduced interoception may report having a high pain tolerance. Sometimes we may not be aware of our interoceptive states, especially whilst we are in hyperfocus mode. To buffer this, it can be useful to set timers to remind us when to eat, go to the bathroom and drink water. Visual prompts are also useful, such as keeping snacks and your water bottle next to you. * Proprioception refers to interpreting our movements, force and position in space. Have you ever had days where you feel like you walk into every possible obstacle, even when you see them? (No, just me again?) Or sometimes you drop your cutlery whilst using it? Or your cat bites you because you are stroking them a bit harder than usual? Sometimes we can feel a bit off during the luteal phase (after ovulation until the bleed starts) of our menstrual periods, and that can stretch out into perimenopause and beyond. Chances are you are not imagining it, and that hormonal flux is affecting your mind and body in ways you didn’t think possible. You might feel like you are literally losing your grip on life, as well as losing your mind. * Menopause is here to show us that we matter - we did all along - but now we can channel our energy into ourselves. I know how scary it is to not feel like yourself any more, to have spiralling cognitive limitations and to think these changes are irreversible. They aren’t, and you will adapt to them, learn new accommodations and, I am assured, come out the other side post-menopausally realising that pre-perimenopause, you were dealing with too many responsibilities, were people pleasing to the max, and put your own needs at the bottom of the list, if at all. * Your brain fog is hormonal, not dementia. There are similarities in symptoms between hormonal brain fog and young onset dementia and, if you are like me, you are likely to make the leap to assume you are on a path of cognitive decline. Neurodivergent people experiencing hormonal flux and decline often feel like they are losing self-care and communication skills. If you are worried about perimenopause, menopause and dementia, you might like to read more here.* Stimulant medications have been shown to help with brain fog in new onset executive difficulties in menopause. For those of us who become overtly symptomatic of ADHD around midlife, trialling stimulants - the first line treatment - may be beneficial. However, access to psychiatric assessment is a major prohibitive factor. * Stimulant medication works for 70 to 80% of ADHDers. Many people find them life changing. They are the most effective medication available in all of psychiatry. It’s now believed to rewire neural pathways and strengthen executive functioning skills longer term, rather than only having the short term effects previously thought of. Here is an informative discussion on ADHD medications.* Non-stimulants can be prescribed whilst awaiting an assessment for ADHD. You will need a doctor who is confident that you present as ADHD based on their professional evaluation in order to trial non-stimulants prescribed off-label. This is useful when a diagnosis is inaccessible, or you are struggling whilst on a long waiting list for assessment. Non-stimulants are the second line treatment for ADHD, and many people who don’t tolerate stimulants do well on them.* All is not lost. Other things that can optimise our executive functioning in challenging times include coaching, body doubling, energy management, pacing and lifestyle factors such as improving sleep. That last one is sometimes the hardest of all, and insomnia can be an early symptom of perimenopause. Often though, ADHD medication and/or HRT/MHT are needed first to boost your executive functioning, energy levels, sleep and mood before lifestyle changes can be made.* Hormone replacement therapy (HRT) can provide a buffer. HRT is not a great name since replacing hormones in most people’s case is not the goal, which is why a preferred term for it is menopause hormone therapy (MHT). Rather, HRT/MHT can provide a buffer to support you from hormone levels dropping so low whilst in flux that they cause unbearable symptoms. Transdermal hormones are safe for most people, and life saving for many. When used alongside other necessary medications and lifestyle optimisation, you can begin to feel like your former self again. Whilst many neurotypicals shout on the socials about how they went from a perimenopausal wreck to a goddess in 24 hours, that is not often the case for those of us who are hormonally sensitive and/or complex. Re-saturating oestrogen receptors (which are located in the brain and every part of the body, which is why menopause symptoms are widespread) can take some time. It is not a miracle cure. HRT/MHT needs tweaks and adjustments to dose and delivery system (e.g. patches, pills, gels or pessaries) under the guidance of a knowledgeable and neuro-affirming menopause doctor. * Taking medication for ADHD and HRT/MHT for menopause isn’t weakness. A so-called natural approach isn’t optimising what your brain can do for itself. We won't receive medals for getting through neurodivergent menopause without appropriate supports, and too many of us don’t make it through alive. We need an individualised toolkit to survive intact, complete with knowledgeable healthcare providers, self-advocacy skills and a network of people who understand, empathise and want to help us. More on self-advocacy and finding the right doctor for you here.What nuggets of wisdom can you share that may benefit us all? I would love to read them in the comments!Click on the ‘view in browser’ at the top of your email and log in if you haven’t already.Behrman and Crockett conclude in their 2024 research paper, Severe mental illness and the perimenopause, that:Discussion of symptoms through the prism of the perimenopause may be helpful for patients in understanding their experiences, and lifestyle advice may help with symptoms, which will have a positive impact on mental and physical health; the same is true for new presentations of perimenopause-related mental health difficulties. If oestrogen levels are balanced with HRT, patients are likely to respond more consistently to medication, perhaps requiring lower doses or less complex regimes and ultimately enjoying better physical and mental health outcomes.Hang in thereYou are already doing your best and, yes, you are good enough! Even when it all feels too hard and all the jobs are unsurmountable, give yourself credit for keeping on keeping on. Then take a break because, if neurodivergent menopause has taught me anything, it’s that most of the expectations placed on me aren’t worthy of my time and energy. So go and have a rest. All $hit good things come to an end, including perimenopause. And thank f$ck for that.Resources, Further Reading and Listening* Professor Russell Barkley’s two episodes (#199 and #200) on the I have ADHD podcast * ADHD for Smart Ass Women podcast* Jessica McCabe’s How to ADHD YouTube channel* Kate Moryoussef’s podcast and webinars https://www.additudemag.com/webinar/adhd-burnout-chronic-stress-women/* ADDitude magazine online and webinarsDivergent Menopause is on a mission to empower, educate and reframe the narrative. Want to support me? The best way is to become a paid subscriber. Your support means the world to me! Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 27m 48s | ||||||
| 11/4/25 |  🎧 1: What is creativity and why does it matter? | I am delighted to be joined by Allegra Chapman (she/her) from Creative Fix!Together Allegra and I have created this four part mini series on the importance of creativity during the menopause transition and beyond.1) What creativity is and why it matters,2) How to fit it in around needs and what activities work for different needs3) Special interests and “accidental” creativity and stuff that’s creative that you don’t think about4) How your creative practice changes as your needs change... or how creativity can help with unmaskingResources:https://www.scienceopen.com/hosted-document?doi=10.13169/intljofdissocjus.5.1.0004Allegra’s bookAllegra’s coursePrevious articles by Allegra? Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 12m 58s | ||||||
| 10/20/25 |  Neurodivergent peri/menopause, PMDD and hysterectomies with Kim Pitts | Content warning: Discussion of suicidal ideation.Themes 💕Hormonal literacy | Mental health | Neurodivergent self-advocacy | Medical gaslighting | Access inequality | Post-surgical recovery | PMDD symptom improvement“When I try to raise awareness — what IAPMD does — their mission is awareness and education.And I think that’s really where any woman or uterus owner should begin: with knowing.I know that’s hard — it’s executive function all over the place — but truly, information is everything.I’ll never forget reading The New Menopause; in it, she says ‘Information is your foot in the door.’And we just — we have to be able to get that foot in the door.Whether you do that through peer support or whatever means you can, that’s one of the only ways right now to really start the conversation.It’s unfortunate, and so tragically unfair.But just know that there’s always a conversation that can be had.We just have to — unfortunately — sometimes be the ones to start it, which is such b******t.But still, there’s always a way to begin.”Kim PittsIf this conversation helps you feel seen, please share or comment below. Your story could help someone else survive their PMDD too.Kim and I have been planning to discuss PMDD and our resulting hysterectomies for a while now, and we finally figured out the timezones between her location of Oregon, US and mine in Wellington, Aotearoa New Zealand.Links to all the resources and further reading we discussed are at the end of this post.Our chat is available in multiple formats for accessibility:* Video with subtitles/closed captions available* Podcast/audio only* Transcription* Plain timestamped summary table** Substack-formatted timestamped summary** Generated by ChatGPT as an executive functioning tool on my part. Sorry, Kim! I know you gave AI the finger during our chat!🩸 PMDD, Hysterectomy & Neurodivergent MenopauseA Conversation with Kim Pitts⏱️ 00:00 – 02:00 | IntroductionsSam (Aotearoa NZ) and Kim (US) open the chat.Both are neurodivergent women who chose surgical menopause (hysterectomy) to stop PMDD symptoms and save their mental health.This is peer support, not medical advice.🩺 02:00 – 04:00 | Surgery StoriesKim shares how her US doctor fought for her right to a hysterectomy despite insurance barriers.Sam reflects on recovery, her four laparoscopic scars, and the strange post-op moment of thinking, “Where’s the baby? Oh wait — no more uterus!”💊 06:00 – 10:00 | Progesterone IntoleranceSam explains how progesterone caused bloating, digestive pain, and depression.Kim agrees—progesterone can be lifesaving or intolerable depending on the body.They unpack the delicate HRT balancing act and how mental health depends on getting the right dose and delivery.🧠 10:00 – 13:00 | Medical GatekeepingSam details the challenge of navigating public vs. private healthcare, using index cards to remember key points at appointments.They talk about executive dysfunction, prescription chaos, and how neurodivergence complicates healthcare admin.💬 13:00 – 17:00 | What Is PMDD?Kim defines Premenstrual Dysphoric Disorder (PMDD) — a neuroendocrine disorder where hormonal fluctuations trigger severe mood symptoms.Often mistaken for PMS, it requires careful tracking, but that’s hard for ADHD and autistic women.📝 17:00 – 22:00 | Hormones, Neurodivergence & TrackingThey discuss multiple hormone sensitivity theory, links between ADHD/autism and PMDD, and why symptom tracking is often impossible.Kim used old text messages as evidence to identify her cycles.⚖️ 22:00 – 27:00 | Self-Advocacy & Self-GaslightingSam shares how she doubted her own symptoms right up to surgery.Both reflect on medical gaslighting, the exhaustion of self-advocacy, and the relief of being believed.Finding the right doctor = survival.⚠️ 25:00 – 33:00 | Suicidality & SurvivalContent warning: Discussion of suicidal ideation.They discuss how PMDD, autism, and ADHD overlap with high suicide rates for midlife women (ages 44-58).They stress the need for hormonal treatment first, not just SSRIs, and for open peer conversation.🫀 36:00 – 40:00 | Hysterectomy Research & HRT MythsKim explains how outdated studies scared women — early hysterectomy patients weren’t given HRT, so they suffered bone and heart issues.Modern practice should include immediate hormone replacement for safety and quality of life.💸 43:00 – 46:00 | Funding BarriersKim shares how she accessed surgery through a hospital financial-assistance program in the US.The approval felt like “relief and disbelief.”They dream aloud of a nonprofit fund to help others afford lifesaving PMDD surgeries.🔄 47:00 – 52:00 | Before Surgery: Life in CyclesSam recalls living between inertia, shutdown, and rage, with shrinking windows of good days.After constant bleeding and progesterone crashes, surgery brought instant hormonal stability and mental clarity.🩺 52:00 – End | Takeaways & Solidarity* Blood tests are a snapshot, not the full story.* Lived experience matters more than lab numbers.* Peer advocacy can bridge dangerous medical gaps.* Both women close with gratitude — for surviving, for community, and for being heard.Resources and Further Reading* International Association for Premenstrual Disorders (IAPMD) website* PMDD Symptom tracker from IAPMD website (above)* The New Menopause - Navigating Your Path Through Hormonal Change with Purpose, Power and the Facts book by Dr Mary Claire Haver* Your Periods, ADHD & the Multiple Hormone Sensitivity Theory Dr Nighat Arif video* MENO-D A rating scale to detect depression in menopause by Professor Jayashari Kulkarni* Progesterone intolerance Dr Loiuse Newson articlePlease take good care of yourself.Want to support me? The best way to support my advocacy and peer support work at Divergent Menopause is to become a paid subscriber. Thank you again for your support! It means the world to me. 💕P.S.: That was intense, so here’s a photo of Harry! I have invested my paid subscriber contributions on some equipment to make my desk more ergonomically accessible post-hysterectomy. Huge thanks to my paid subscribers for making this possible! Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 1h 11m 17s | ||||||
| 10/17/25 | 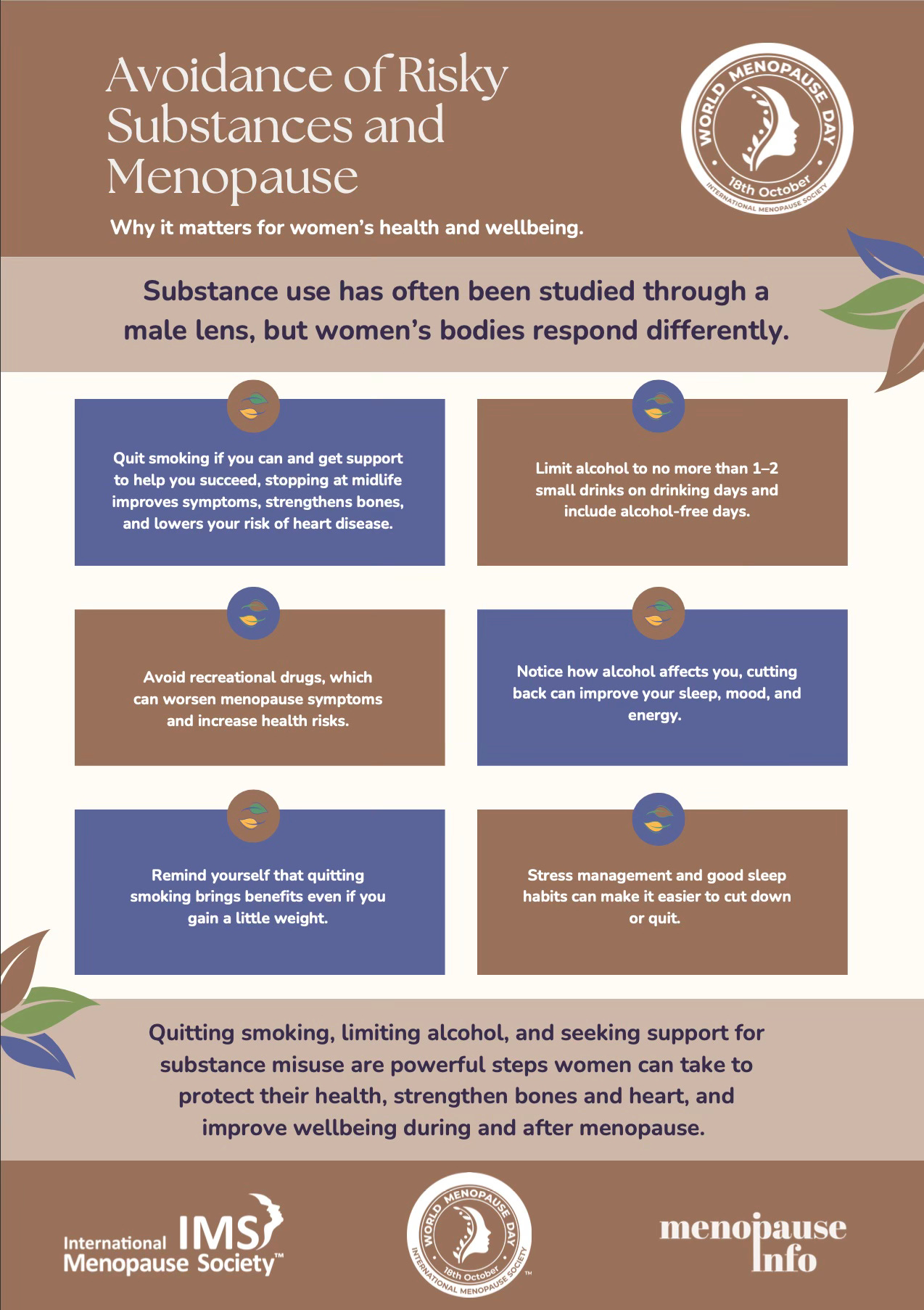 Happy World Menopause Day 2025! | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression.I am Sam Galloway (she/her) and I am an AuDHD woman seven weeks into surgical menopause (hysterectomy).If you are interested, you can read more on why I needed the surgery here.Thanks for joining me on this wild midlife ride! 🎢October 18th marks the annual event that is World Menopause Awareness Day! In this video and podcast episode, I take you through the advice (see the six posters below and here) provided by the World Menopause Society for 2025’s theme of Lifestyle Medicine in Menopausal Health!Closed captions and transcript available too.🎥 Prepare yourself for much brain fog, sarcasm and despair as I explore the multiply astonishing ways in which this mainstream advice is, at best, inaccessible and, at worst, detrimental to neurodivergent people going through this life transition. 🎧Here is last year’s World Menopause Day post from me.Some resources referenced in the video/podcast today:I wrote this article on Blue Zones earlier in the year, because I have always been obsessed with longevity research. However, I am now extremely scornful on the topic as you will find out if you read this, or listen to the podcast episode link in the following post:This is a great read on the narrow minded push for Mediterranean style diets:The six (!) International Menopause Society posters I share in the video, brimming with unreachable targets for so many of us who don’t and can’t conform to neuro-normative expectations:Below is my viral 2024 post, which shows that our way of being in the world is totally valid and important. Maybe we need anti-goals for menopause lifestyle advice. What would yours be? I would love to know in the comments.Take good care of yourself. 💐And be realistic about it, the above International Menopause Society goals were not written with neurodivergence, chronic illness and disability in mind.Cheers,Divergent Menopause is a labour of love. Each article takes hours to research, write and edit. If you have found my ongoing advocacy work valuable, please consider becoming a paid subscriber if you are able to. Thank you 💕 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 43m 40s | ||||||
| 9/27/25 |  Part 4: Nervous System Regulation in Neurodivergent Menopause | Hello and welcome to Divergent Menopause, previously known as The Autistic Perimenopause: A Temporary Regression. I am Sam Galloway (she/her) and I am an AuDHD woman four weeks into surgical menopause (hysterectomy). If you are interested, there is more on why I needed the surgery here. Thanks for joining me on this wild midlife ride! 🎢Hi All, Welcome to the final video of the mini series with Amanda Hanna from SomaPsych. I hope you have enjoyed it! Please let me know in the comments whether you like this format, and what topics you would to see covered in future mini series. This episode requires a content warning for suicidal ideation and actions, panic attacks, mental health crises and feelings of hopelessness. So many helpful techniques offered, and I would love to know which, if any, you find most effective. Please let us know in the poll, and feel free to expand in the comments. In case you missed the previous videos, the first offers techniques to use in the margins of our day to regulate our nervous systems and feel rested. In the second video Amanda suggests how to stop anxiety spiralling at night and (hopefully!) get back to sleep. The third video covers how to manage chronic pain flares and reduce recovery times.Why do we need S.O.S. techniques for de-escalating sudden panic, suicidal ideation and feelings of hopelessness?In my experience of pre-menstrual dysphoric disorder (PMDD), pregnancies, postpartum, puberty and perimenopause (not listed here in chronological order), states of hormonal flux trigger extremes of mood and personal safety concerns.Now that I am in a state of surgical post-menopause by hysterectomy, and in the fresh absence of my ovaries, my hormone production has now flatlined. That was the intention of my highly medicalised menopausal treatment plan, in order to eliminate all risk to myself from my own hormonal fluctuations.Some people may have lovely menstrual cycles and manage their perimenopause with minimal medical interventions. I am genuinely happy for those people, and wish we could all be like that. But we can’t. Some of us experience sudden moods that are so inextricably linked to our extreme hormonal highs and lows, that we cannot understand why we think we would be better off dead before we have had time to challenge that thought. For autistic women, our suicide risk is 13 times higher than that of neurotypicals during midlife. 1 in 4 ADHD women have attempted suicide. Perhaps, like me, you are an AuDHDer. I don’t have the stats on us, but I expect they are bleak. I don't tell you those statistics to shock or frighten you. My intention is to make you aware that you may be at increased risk, but that you have the ability to mitigate that risk by being aware of your emotional states throughout times of hormonal flux. We can be extremely impulsive, which may have been great when we were younger, but we have so much more at stake in midlife. If your highly sensitive brain tricks you into thinking your rage is shameful and your family would be better off without you, please know that that is a common thought. We just don't live in a society where it is acceptable to share these thoughts with someone else. I get DMs from people frequently who are feeling this way.Our thoughts are not facts, they can’t objectively dictate to us. Thoughts come, and then they go, and new ones take their place. Please share with others if you are experiencing thoughts of suicide, self-harm or causing harm to others. Ruminating on these thoughts isn’t unusual, and just because certain thoughts persist and/or recur doesn’t make them any more substantial or credible. You matter to me, to this community and to all the people who love you. Sometimes it doesn't feel like this, I know. During perimenopause I too experienced intrusive thoughts that put my family and I at risk. Thoughts that I should stop my car on the train tracks and wait for a freight train to stop my pain and functioning regressions. My kids were in the back of the car! And it was a recurrent thought.Often I wasn’t even experiencing suicidal ideation until I reached a railway crossing, and that would trigger the thought. I would hum, stim, flap all whilst driving; trying to hush and force away the thought, consciously accelerating across the tracks and willing myself to stay in motion on the road. It took all of my limited energy to just get my kids and I home safely, at which point I would need to crash (excuse the pun) out on the sofa. Often autistic inertia followed. It would take me 24 hours to process the thoughts, which had come and gone in the fraction of a second, and to tell my husband and/or my doctor what had happened. I don't wish that pain on you. It can be common in neurodivergent menopause, but please, let’s not normalise it. It is a signal that you need more support, more rest, more mental health interventions - and those aren’t bad things. As late diagnosed neurodivergent, we have stuffed down our feelings for decades. This is the time to unmask, to reach out, to prioritise yourself. For me, this looked like surgical intervention to stop the problem at its root cause - by cutting out my ovaries the surgeons have stopped my hormonal flux. Yes, it is drastic, but not as drastic as the potential headline “Local woman, 44, and two sons killed on impact by freight train”. Please, take your thoughts to someone else if and when they are bothering you. I am not saying a hysterectomy is the answer for you, but I know for sure that suicide definitely isn’t. Please don't underestimate the power of a safety plan! Contrary to popular belief, talking about suicide does not lead to suicide. If you are experiencing suicidal ideation, self-injurious thoughts or behaviours, and/or fear for your own or someone else’s safety, please tell someone you trust. Although overwhelmingly intense, these feelings do pass. Get help now to protect your future self. Zoom AI has provided the following summary of the conversation:SummaryManaging Panic and Suicidal IdeationSam and Amanda discussed techniques for managing panic, anxiety, and suicidal ideation, particularly in the context of neurodivergence and hormonal fluctuations. Amanda emphasized the importance of recognising patterns and creating a "rescue kit" with soothing objects and practical items like water and medication to help manage overwhelming moments. They also highlighted the need to remember that these experiences are temporary and to practice self-compassion during difficult times.Safety Planning for Panic ManagementAmanda and Sam discussed strategies for managing panic attacks and creating safety plans. Amanda shared her methods of using post-it notes and voice recordings as reminders during overwhelming moments. Sam mentioned a video she created on writing autism-adapted suicide safety plans, emphasising the importance of considering professionals' availability and boundaries. They both stressed the value of evolving safety plans and having prearranged signals with supportive contacts for distraction or reassurance.Mindfulness Tools for OverwhelmAmanda discussed the challenges of managing overwhelming situations without proper safety resources, explaining how the brain can become hyper vigilant or fixated on past or future concerns. She described various personal tools people use to ground themselves in the present moment, such as physical sensations or specific activities, and emphasised that finding an effective tool requires personal discovery. Amanda concluded that these tools serve as circuit breakers to help individuals regain focus and presence.Neurodivergent Emotional Management StrategiesAmanda and Sam discussed strategies for managing intense emotional states, particularly focusing on post-panic attacks and suicidal ideation. Sam shared her experience of having suicidal thoughts while driving, particularly during hormonal fluctuations, and emphasised the importance of having a plan for dealing with such moments. They agreed that it's crucial to recognise these feelings as part of their neurodivergent experiences and to consider the impact on loved ones, rather than acting impulsively. Amanda highlighted the need for more open conversations about these experiences, especially in neurodivergent and hormonal contexts.Emotional Regulation Techniques DiscussionAmanda and Sam discussed tools for managing discomfort and panic attacks, with Amanda introducing "riding the wave" as a technique for observing and navigating emotional states without immediate action. Sam shared personal experiences with ADHD and autism, highlighting how pattern recognition can both help and hinder understanding of emotional responses. They agreed that building nervous system regulation capacity through regular practice, even when feeling well, is crucial for better managing challenging moments.* Toolkit: Warning Signs of Suicide for Autistic People: An autism-specific resource based on research findings and expert consensusPlease take good care of yourself. Cheers, If you find my work valuable, why not become a paid subscriber to The Autistic Perimenopause: A Temporary Regression? (This is not a rhetorical question.) Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 21m 10s | ||||||
| 9/20/25 |  Part 3: Nervous System Regulation in Neurodivergent Menopause | Hi Team Auti Peri, Welcome to the third video in the series with Amanda Hanna from SomaPsych. In this episode we explore how to:* identify our individual patterns of current or recurrent pain flares* be present at times of reduced pain or “good moments”* encourage the nervous system to imprint soothing and regulating patterns in our bodies.How does the nervous system get to know what is painful? What is uncomfortable? What’s tension versus tightness? Please share in the poll which techniques discussed in this video that you have tried. I suspect this work needs to be done consistently and regularly to see longer term benefits. The poll has been set to stay open “Forever” (which feels like more time than we need), so feel free to come back to this episode in the future and let us know in the poll and the comments what benefits you have noticed over time. In case you missed the previous videos, the first offers techniques to use in the margins of our day to regulate our nervous systems and feel rested. And in the second video Amanda suggests how to stop anxiety spiralling at night and (hopefully!) get back to sleep.Amanda discusses the work of Addie deHilster (she/her), Founder of Moved To Meditate. Addie is a Mindful Movement specialist who offers “Mindfulness practices for all the moving parts of your life”. To explore her work into meditating and moving with pain, you may like to listen to these podcast episodes:We'll cover:* the discomfort that is a normal part of the meditation process* meditating when the pain is more serious or ongoing* what the research says about mindfulness and pain* how the practice might need to be adjusted to accomodate painWhat you’ll hear about chronic pain and yoga:* defining chronic pain and what makes it so complex* how Yin Yoga practice can help you unwire habits and beliefs that perpetuate pain* using Somatic exercises and Yin poses to build back confidence in movement, and decrease fear* how Yin Yoga contributes to restoring your body image if it has been distorted by prolonged pain experiences.You’ll hear about:* addressing social anxiety and sensory issues that can come up for neurodiverse meditation students in a class setting* the importance of offering multiple ways to practice a technique like Mindfulness of Breathing or Loving-Kindness Meditation* stacking anchors to help students connect with the kinesthetic, visual, or auditory aspects of meditation, on their own terms* being aware of how different verbal instructions may (or may not) work for everyone* how Sue and Jan approach mindful movement or walking meditation for neurodiverse groups.In this video we are lucky enough to have a star cameo from Amanda’s puppy, Layla! ⭐️ 🎥 🐕🦺 Zoom AI has provided the following summary of the conversation:Conversational Discussion on Puppy FascinationSam and Amanda engaged in a casual conversation, discussing a puppy named Layla who was under the desk and seemed fascinated by a light. They briefly talked about taking notes and the appearance of a quill, before Sam prepared to record a video.Chronic Pain Management StrategiesSam and Amanda discussed strategies for managing chronic pain flares and reducing recovery times, particularly for neurodivergent individuals. Amanda shared insights from Addie deHilster's work on chronic pain management, including the concept of pendulating between neutral and painful sensations to help the nervous system reframe pain experiences. They explored techniques such as using opposite sensations (e.g., cold for hot pain) and planning ahead to mitigate predictable pain triggers. Sam emphasised the importance of explicit instruction for neurodivergent individuals, who may not naturally associate physical sensations with emotions.Shoulder Pain and Hypermobility JourneySam discussed her experience with shoulder pain and her journey to understand its root cause, which she suspects may be related to hypermobility and potentially Ehlers-Danlos syndrome. She explained that traditional medical approaches, like physiotherapy, might not address the underlying issue and highlighted her self-discovery process about "coat hanger pain," a term she learned that describes a specific pain region.Chronic Pain Management StrategiesSam and Amanda discussed strategies for managing chronic pain, focusing on balancing periods of pain and wellness. Amanda emphasised the importance of being present during "good" moments to help the nervous system better process and remember these feelings, which can help reduce the perception of pain over time. They also touched on how certain hormones and neurotransmitters, such as dopamine and serotonin, play a role in regulating pain and mood. I hope you have enjoyed this episode, and the series so far. The next episode concludes this mini series on nervous system regulation.Wishing you a regulated week!Cheers,The Autistic Perimenopause: A Temporary Regression is a reader-supported publication. Subscribe so you don’t miss a post, and please consider supporting the ongoing advocacy for neurodivergent menopause by becoming a paid subscriber. Thanks! Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 14m 08s | ||||||
| 9/19/25 |  From Auti Peri to Divergent Menopause | 📣 Great news! The Autistic Perimenopause: A Temporary Regression has been renamed Divergent Menopause. Yay!! 💕It’s less of a mouthful, for sure. Only the name has changed, it is still me - Sam Galloway (she/her) and my faithful ragdoll cats Harry and Toby - steering the good ship Divergent Menopause. TL;DRWhy “Divergent”? Inclusivity.Why “Menopause”? Verb, not noun. To cover the entire menopause transition and beyond. Why the rename? For the sake of inclusivity for all our differently wired neurokin.Most autistic people have other co-occuring neurodivergent conditions, such as ADHD, sensory processing disorder, dyslexia, dyspraxia etc. Although we may not be aware of them all yet… Not all neurodivergent people will identify as autistic, but they may be having a scary old menopause transition, sharing most, if not all, of the same struggles and challenges. Let’s build each other up! We all know that the academic research is unable to keep up in real time with what we are uncovering daily about the ways our menopause experiences diverge from “the norm”. I believe that research will soon catch up and uncover that all of us differently wired legends share similar strengths, vulnerabilities, support needs, cognitive regressions and so on. I also believe that in time rigorous academic research will show that neurodivergent people are more likely than neurotypicals to have hormonally sensitive bodies and minds, and that we are collapsing under the weight of extreme hormonal flux.While they are piecing it all together, running research projects and publishing evidence that will take even longer to disseminate into supporting the everyday challenges faced by neurodivergent people, we are already gathering here. Our stories matter. Every time you leave a comment, reply to someone else or generously share your story in the Auti Peri Q&A (yet to be renamed…) feature, you are helping to compile the anecdotal evidence of what it means to move through the menopause transition neurodivergently. I could not do this work without you. We are trail blazers! This is urgent now. Autistic midlife women are 13 times more likely to attempt suicide than non-autistics. 1 in 4 ADHD women have attempted suicide. Compounding a lifetime of high masking neurodivergence with menopausal hormonal flux exacerbates our vulnerability. We already have lower than average life expectancy. The sooner we understand the risks our differences can present, the sooner we can engage appropriate support systems and maintain our safety. As neurodivergent people, I believe that we need to group together rather than being siloed by our different diagnoses. We have more in common than we have differences. Also, and I know I am not the only one, I am BOTH autistic AND have ADHD. An AuDHDer.Additionally, I have diagnosed anxiety, undiagnosed hypermobility/connective tissue disorder, dyspraxia, dyscalculia, and other neurodivergences that I can’t even recall right now thanks to my major menopausal and post-general anaesthetic brain fog…In my pre-peri life, I was likely gifted which is a yet another form of neurodivergence, but my cognitive regressions have raged on and on regardless of management of other symptoms. I hope it’s reversible as I age…Although my ADHD and autism have both been late diagnosed, when I look back over my life I can see eras where one reigned over the other. Often it was the ADHD that ramped up in times of pre-peri hormonal flux, such as during puberty. Then something about being a mother made me present more autistically overall. Yet I was multi-neurodivergent all along.Separating my neurodivergences is fruitless, I can no longer pretend to be more one than another. They all contribute to create the mess the person who is writing these words to you right now. It feels increasingly inauthentic to present my writing purely from an autistic perspective, when I am an AuDHDer, with astonishing levels of executive dysfunction to prove it. I don’t want to be down on my autism, my ADHD, or on any of the other complexities that make me me who I am. And so in renaming this community Divergent Menopause I hope that we continue growing in numbers, diversity and momentum. There are so many things I need to iron out, but I can’t right now because my brain is mush. Three weeks post-hysterectomy feels like an entire lifetime and a fleeting moment. I have been told by the surgeon and my primary care doctors that the recovery time is 6 to 8 weeks, and also that the general anaesthetic may take 3 months to wear off entirely. That means I am hopeful to be pain-free, fully mobile and have clarity of mind just in time for Christmas, which will be a gift. 🎄The reason I am calling this move a “rename” rather than a “rebrand” is because Canva looked at my efforts for a new logo and told me to stop wasting both our time. Here are some examples *cringe*And why have I changed the name from Perimenopause to Menopause?Simply because I have transitioned from a perimenopausal state to a surgically induced post-menopausal state in the slice of a scalpel (well, several, I have four incisions…).I am fully aware that the word ‘menopause’ is generally used as a noun, with the dictionary meaning of being the day that is exactly one year after a person’s final menstrual bleed. Yet menopause does not often fit into tidy little boxes. I haven’t had a menstrual cycle since I had a Mirena IUD inserted two years ago this month, and that was only advised because I was having a constant uncontrollable bleed that lasted months. I wouldn't call that a “period”, but we don’t have words for that either. The bleeds I have had since have been short, isolated emotional bodily trauma responses. One occured at my Dad’s deathbed, the other when my Mum’s visit to stay with my family in Aotearoa New Zealand ended and she went back to the UK. My GP advised me to anticipate another bleed in the event of any future little-t trauma. Hormones impact our emotions. Emotions impact our hormones. We are not as straightforward as medical science would like us to be, hence decades of gross negligence into avoiding research on women’s health. I am your classically annoying correct autistic pedant. I know that the language around the menopause transition is deliberately blurred. We descend from generations of women who were not supposed to talk about their menstrual bleeds, nor their cessation. We may never have heard from our sisters, cousins, aunties, mothers and grandmothers on the subject of hormones and menopause, and we were socialised to be “good girls” by not asking questions. The language of menopause, even our own anatomy, has been denied us. Our neurodivergent ways of communicating go chronically misunderstood and silenced. When we have questions in midlife, medical science does not yet offer answers to our predicaments. None of this is our fault though, and Divergent Menopause will continue to be a safe space for us to chat about our lived experiences. This remains a community that welcomes all forms of diversity. For all these reasons, my use of the latter word in the new name Divergent Menopause will be intended as a verb, rather than a noun. “Menopause” as an occurrence, a state of being, a transitional time in our lives. As for the Auti Peri Q&A, I still welcome people to please forward their responses to me if they would like to feature in the series! 🙏The Auti Peri Q&AI will soon be adapting the Q&A questions to open it up to all neurodivergent people who would like to share their experience of the menopause transition. I have other grand plans: to start a proper podcast, to rebrand Divergent Menopause with Autumnal tones, and perhaps to one day train as a menopause doula.But that is all going to have to wait until my brain is fully functioning again.🤞I thought I would have moved on from that stage in three weeks, but I suppose major surgery is major surgery… It is reminiscent of how I was feeling whilst still in hospital. ⬇️As I type this, my homemade hysterectomy pillow is lying across my tummy and under my arms giving me oodles of support, as I hoped it would. My laptop is balancing precariously on top of it. I have also been building this amazing LEGO set I was gifted to build whilst recovering from surgery. The wooden tray has also been balanced precariously on the pillow during the extensive build!I hope the name change isn’t too much of a shock. I hate surprises and change, and even I am cringing at the new name, despite it being a change I have been intending to make for many months now. It would be great if you could please share Divergent Menopause within your networks to help us get more visibility, have a wider reach, and, in so doing, support more people to feel less alone and lost in the haze of this challenging yet unavoidable life transition. I think it’s time for another nap…I hope you have a restful weekend ahead. Take good care of yourself.Cheers,Divergent Menopause (formerly known as The Autistic Perimenopause: A Temporary Regression) is a reader-supported publication. Paid subscriptions are on a patron model. If you find my work supportive and informative, and you value advocacy work, please consider becoming a paid subscriber. Thank you! 💕 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 13m 27s | ||||||
| 9/12/25 |  Part 2: Nervous System Regulation in Neurodivergent Menopause | Hello to you, Welcome to the second part of this four part video series with Amanda Hanna from SomaPsych. You can watch Part 1 here. In the first video we discussed techniques to use in the margins of our day to regulate our nervous systems and feel restedThis time we focus on sleep, which can be so elusive to neurodivergent people in times of hormonal flux. Let’s face it, sleep can be hard for us throughout our lifespan. As children, we may have formed negative associations with sleep depending on how gently - or not - our own times of sleeplessness were managed. This can impact us as we age. I know I can’t be the only midlife neurodivergent parent having to co-sleep with a child to give the whole family a better chance of refreshing sleep. This comes at a cost to me though, as flailing limbs of pre-teens does nothing to help with night sweats and hormonal insomnia…Resting during the daytime can be a challenge for us too, as high anxiety coupled with executive dysfunction can make everyday tasks take ten times longer - if we can do them at all. Writing “Take a nap” on our to-do lists rarely leads to action (or inaction in the case of napping?).But don't despair! Amanda is back with more neuro-affirming gems to help us learn to soothe our nervous systems, increasing our chance of improving our sleep overnight rest opportunities (sometimes calling it “sleep” just adds too much pressure).In Part 2, Amanda encourages us to ask ourselves:“Are there restful things I could do in the moments when sleep is not happening?”So many helpful techniques offered, and I would love to know which, if any, you find most effective. Please let us know in the poll, and feel free to expand in the comments. Let’s collectively workshop sleep for everyone’s benefit!As always, the transcript and closed captions are available to ensure the video content is as accessible to you as possible. If you prefer audio only content, you can listen to our chat as a podcast episode. 🎧Zoom AI has provided the following summary of the conversation:SummarySleep and Anxiety Management StrategiesSam and Amanda discussed strategies to manage anxiety and improve sleep, particularly for neurodivergent individuals and those experiencing hormonal shifts like perimenopause. Amanda emphasised the importance of reducing cortisol levels to allow melatonin to work effectively for sleep. She suggested techniques such as journaling, soothing activities, and setting restful associations through lighting cues. Sam shared personal experiences with sleep disruptions, including urinary incontinence and mast cell activation syndrome, and highlighted the importance of understanding body signals to manage waking up at night.Open Monitoring and Brain RestAmanda discussed the concept of open monitoring, which involves allowing the brain to daydream and wander, particularly during moments of low external stimuli. She explained how the hippocampus, often compared to a librarian, processes and files away memories when the brain is not actively engaged. Amanda emphasised the importance of giving the hippocampus time to clean up and organize memories, contrasting this with the constant demand for productivity and attention in modern society. Sam acknowledged her difficulty in allowing for such moments of mental rest.Short Meditation Practices DiscussionAmanda and Sam discussed incorporating short meditation practices into daily routines, such as 30-second mindfulness moments and a figure-8 eye movement exercise for sensory stimulation. Amanda explained that these techniques can help reduce stress and improve sleep, while Sam expressed interest in trying the eye exercise that night. I hope you enjoyed the second part of this mini series. We are already halfway through. I can’t wait to share the next two instalments with you!Cheers, The Autistic Perimenopause: A Temporary Regression takes extra effort to write and curate whilst recovering from major surgery. Show your support by beco ming a paid subscriber, so you can glow inside knowing that you are a patron of neuro-legendary menopause advocacy! 🌟 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 13m 41s | ||||||
| 9/5/25 |  Part 1: Nervous System Regulation in Neurodivergent Menopause | Hi Team Auti Peri!Well, here it is! The first part of four in this series on nervous system regulation, yay! I would like to take this opportunity to once again thank the lovely Amanda Hanna of SomaPsych for sharing her time and expertise with our community. At SomaPsych, we empower resilience and transformation through trauma-informed care and somatic practices - from individual restoration to collective social change.Amanda weaves science with embodied wisdom, crafting spaces where curiosity thrives and empowerment takes root. Her approach is nervous system focused, polyvagal informed, collectively-minded and grounded in a deep reverence for all things ecosomatic and alive.I am still lying flat on my back in bed after my hysterectomy last week, so I have included the Zoom AI meeting summary below (demarcated in block text) as the main body of the article. At the time of recording I had fully intended to write up a lovely summary for you, but now I am unable to even sit up unaided. Plus my painkillers make it rather difficult for me to convey much coherence!I know AI usage is contentious, but needs must. I need my recovery to be as smooth as possible as I have regressed so far within the bowels of my neurodivergent perimenopause, and now I need to cut myself some slack.Please be assured that the video conversation is real though, ha ha! You will be able to tell that from my inability to cut out the first three seconds. Oh I had such grand plans of making this mini series look slick and professional. Sigh..!As always, the transcript and closed captions are available to ensure the video content is as accessible to you as possible. If you prefer audio only content, you can listen to our chat as a podcast episode. 🎧After you have watched the video, please come back and let us know in the poll which technique is helping you the most. Quick recapSam and Amanda explored nervous system regulation challenges, particularly for neurodivergent individuals, and shared strategies for managing mood fluctuations and emotional responses. The conversation concluded with Amanda providing coaching on managing difficult thoughts and building a relationship with the amygdala, with plans to continue their discussion in future recordings.Neurodivergent Nervous System Regulation ChallengesSam and Amanda discussed nervous system regulation, particularly for neurodivergent individuals who have spent their lives masking and managing their emotions. Amanda explained that nervous system regulation involves understanding both internal and external sensations, and recognising when one is in a "green zone" of relative calm versus experiencing dysregulation. They agreed that the constant pressure to maintain regulation can be particularly challenging for neurodivergent people during menopause, when control may feel even more elusive.Enhancing Well-Being Through Daily ToolsAmanda and Sam discussed strategies to manage nervous system regulation and mood fluctuations, focusing on integrating simple tools and techniques into daily routines to enhance well-being. Amanda emphasized the importance of "stacking" these tools during everyday activities, such as filling a water bottle or making tea, to create moments of calm and downregulation. She explained the concept of physiological sighing as a natural technique to shift brain chemistry and reduce stress. Sam shared personal experiences with mood stabilising medication and expressed a desire to rely more on self-regulation techniques. Amanda concluded by demonstrating a physiological sigh, highlighting its effectiveness in promoting relaxation.Self-Regulation Techniques for Emotional ControlAmanda and Sam discussed self-regulation techniques, focusing on both public and private methods for managing emotional responses. Amanda explained that she uses both overt and covert strategies, including physical gestures like palm massage, to maintain control in different situations. She emphasised the importance of having both visible and hidden coping mechanisms, allowing her to manage her emotions without always needing to explain herself to others.Amygdala Regulation and Thought ManagementAmanda provided coaching to Sam about managing nervous system regulation and dealing with difficult thoughts, explaining that the amygdala's role is to keep us safe and suggesting that building a relationship with it can make challenges easier over time. They discussed how rumination can lead to hyper-focusing on negative thoughts, and agreed to end the current session with plans to continue in the next recording. I hope you enjoyed the first part of this mini series. I can’t wait to share the next three instalments with you!Cheers, If you find my work valuable, why not become a paid subscriber to The Autistic Perimenopause: A Temporary Regression? (This is not a rhetorical question.) Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 15m 59s | ||||||
| 7/25/25 |  Burnout Prevention at The Autistic Perimenopause 💕 | Dear Team Auti Peri, Thanks for being here, your presence means the world to me!Contents summary* Why I am taking August off* Things you might like to do to contribute at The Autistic Perimenopause* Exciting plans for September on nervous system regulation in neurodivergent hormonal flux with sneak preview!* Recap of the Autism Adapted Suicide Safety Plan with links to the Newcastle University document, and my previous video and audio step-by-step guide* Bonus content only in this audio recording: A real life cat fight between Harry and Toby when my son accidentally let them into the recording room to tell me that Harry had knocked over a plant pot in the kitchen. With cat squeals and inaudible flying fluff! Note to self: go and clean up the plant pot mess. With any luck, the cats won’t have peed on the soil/carpet… 🪴 🙄🐈 🐈⬛ 🐈 🐈⬛ 🐈 🐈⬛ 🐈With reluctance, I have decided that I need to take some time off to focus on my own health and wellbeing. It won’t be for long! A few weeks ought to do it. My little family is in desperate need of a holiday (vacation/break/total reset), and I haven’t taken any time off from The Autistic Perimenopause: A Temporary Regression since it launched in April 2024. So I am planning on taking off all of August for a personal mental health break. This is a one woman show, and this one woman is at risk of cracking up entirely. I fear if I breakdown completely this time, I may be unable to piece myself back together. If you are familiar with my work, you will know that I am adamant that a neurodivergent menopausal transition can be a distressing and prolonged time for many of us. I don’t know about you, but every single time I spiral further downwards at an alarming rate, I wonder if I ever will be able to reverse these regressions. I want so badly to make sense of my own menopause in the way aspirational writers do: the ones who tell us that this is an opportunity to live the second half of our lives with joy and purpose. They say, once we become empty nesters, we can invest our newfound time entirely in ourselves. This theory of the menopause in no way aligns with my lived experience. Those of us who suddenly find ourselves in neurodivergent perimenopause, often only uncover our neurological differences alongside our children’s diagnoses. Our midlives are lived outside the norm.We may not have an empty nest to look forward to. We are often devoted parent carers: we prepare different meals for everyone in the home to ensure safe foods are always available; we monitor and despair at our kids’ ever increasing screen time (just me?); many of us choose to homeschool - due to the failure of the mainstream schooling system, or from personal preference. For those of us who have neurodivergent kids in schools, we may find ourselves constantly meeting with teachers and special education needs coordinators (SENCOs), feeling belittled and blamed when our children naturally react to the school systems’ inability to accommodate them all of the time. And what about when our differently wired children grow up? With their spiky profiles and asynchronous development, they may not be equipped to leave home at the same time as their non-disabled, neurotypical peers. Yes, we strive for them to be independent. We see their pure brilliance. We want them to be happy, and preferably not gaming into their 30s in our basements, needing regular reminders to clean their rooms of dirty dishes and even dirtier laundry. And - for goodness sake - can’t they just take a shower AND apply deodorant without being verbally badgered to do so? Our families are often on a different trajectory entirely from regular families, which is why it cuts so deep when others have no awareness of the extra effort we put into helping our offspring assimilate into this world that does not have their best interests at heart, to say the very least. To be told that we are pandering, enabling and just plain parenting wrong is insulting. And it most often comes from those we love, rarely from the psychiatrists, therapists and support workers who are privy to the most intimate details of our volatile and tender day to day lives. Well, I don’t know where that came from, because I went completely off topic. How cathartic though, ha ha! Anyway, yes, I suppose I do need a break because of all the stressors above - perhaps you do too? - and also: * Down here in Aotearoa New Zealand we are months into the depths of Winter, and my body hurts from the cold. It is hard to motivate myself to get outside and I am quite possibly depleted of Vitamin D. I haven’t looked into this, but I had a B12 injection last week and am hoping to recover some energy soon. * My brain fog is absolutely off the charts, I can barely hold a conversation in person. I have loads of half written posts drafted, and not enough cognitive capacity to feel they offer you enough value to publish yet. I am extremely keen to get an article out to you on the topic of progesterone intolerance, but for the life of me I cannot remember what my lived experience of it has been. Which is ridiculous, as it is one of the reasons that I was recently approved for a hysterectomy! And I have no idea of the timescale for my upcoming surgery, which is very difficult to deal with as an autistic woman, especially with full time homeschooling parent carer duties and extremely limited respite and childcare options. * I am being treated for mast cell activation syndrome (MCAS) which is definitely exacerbating the brain fog and have started the antihistamines (H1 and H2 blockers). My body is in a state of alarm at all times, and I need to learn about the histamine elimination diet that can help my body and mind recover from the onslaught it perceives from stress, my regular diet and lack of refreshing sleep. Ironically, the MCAS-induced brain fog precludes me from understanding the complex underpinnings of a low histamine diet, which may be the primary way to combat the brain fog… But the MCAS is insisting that I rest, and I need to obey in order to reassure my nervous system that I am safe. * I have recently realised that I am most likely hypermobile and am now highly symptomatic with pain flares, ongoing gastrointestinal issues and worsening proprioceptive challenges. I think this is all highly pronounced now that I am around nine months into a chemical menopause, although I was probably asymptomatic hypermibile until now. I have signed up to The Zebra Club app for community, hypermobile-friendly workouts, and hours and hours of presentations to try and understand how to soothe my nervous system and understand my body’s needs, strengths and limitations. I have an unstable shoulder joint, currently aided by kinesiology tape, and have just taken delivery of my new firm compression tops to help with stability and proprioception. Basically, I am having to unlearn everything I thought I knew about how to move, sit, stand and so on, and relearn where my body is in space, how to stop bracing my muscles, and keep my joints within their safe, painless range. * If I were in a conventional employment arrangement, I would have statutory holiday leave entitlement. But it’s just me and my phone, and we are in a very compulsive, strained and unboundaried working relationship. Thanks to ADHD, I am “all or nothing”. Rather than the default being all in on my work, I need to switch over for a short time into going all in on rest. * The Substack gods are getting in my head, and I need to show them that I am in control of my own mind (which I am hoping turns out to be the case). My subscriber numbers are down, both free and paid, with paid rapidly approaching single digits. I need to stop checking the stats and break that habit. I love all my readers and subscribers, free and paid, and would find it extremely validating to find my paid subscriber numbers increasing. But I have zero control over that, and hope that people are finding value in my work regardless. I still offer everything for free and I would like to continue to avoid paywalling content that people may need and can’t afford to pay for at this time. Thank you to my paid subscribers for supporting all my hard work! 💐* I know we are all crazy busy and super stressed - my troubles listed here are far from unique and pretty minor on the grand scheme of things. I don’t currently have any more Auti Peri Q&A interview posts to publish because I haven’t received any responses lately, which is totally understandable. I am always seeking more Auti Peri Q&A respondents (here’s why), so please reach out if you are keen to participate.* A personal goal is that I would like to launch a proper podcast about neurodivergent menopause, to interview experts and advocate on a larger scale. I have been lucky enough to free up a room in my house which will soon become my writing and podcasting room. It currently houses many of my houseplants, a lot of my LEGO sets and a dumping ground desk already cluttered with paperwork. It is far enough up the hallway from where my kids play online with their friends, screaming and laughing, to hopefully not pick up too much background noise. I need to somehow sort out some optimal acoustic panelling or something before I can get started though. Oh and find guests. And create an intro/outro, find music, childcare *Sam enters major overwhelm…*🐈 🐈⬛ 🐈 🐈⬛ 🐈 🐈⬛ 🐈Here’s what you might like to doHave you listened to any great podcast episodes lately about autistic perimenopause, read any academic papers, or watched an insightful webinar on YouTube? If so, please share the links to any new credible, academic or informative resources about autistic perimenopause and beyond in the comments of the 💕 Resource Roundup 💕 page which was last updated in October 2024. (Or any links to older stuff that I missed!) If you are reading in the Substack website version, you can find it in the tab headings here:* Have you explored the archive at The Autistic Perimenopause: A Temporary Regression yet? 📣 Did you know?All my previous posts are available for you to read in the Archive section of my publication at any time.There are now over 100 articles in the Archive, including lots of Auti Peri Q&As sharing the stories of a range of lived experiences. Because autistic perimenopause isn’t doom and gloom for everyone, luckily!“There is so much value in the Archive!” affirmsClaire Venus ✨If you are interested in a particular topic on intersecting neurodivergence, mental health and/or all things midlife and menopausal that I may have previously covered, you can search the Archive 🔍 as shown below.First select the Archive (as circled in the photo) in the navigation bar, then click on the Search function (starred in the photo):Nothing is paywalled on purpose because I don’t want financial barriers to anyone accessing the information, personal stories and community I am creating here on Substack around autistic menopause. I would be so grateful if you would support my work by becoming a paid subscriber.🐈 🐈⬛ 🐈 🐈⬛ 🐈 🐈⬛ 🐈Normal service will resume in September, and I am so excited to have a four part video series to share with you. Yesterday I was lucky enough to spend time with the amazing Amanda Hanna from SomaPsych. We have collaborated on four short video sessions that I will share with you each week in September, with a focus on nervous system regulation in neurodivergent perimenopause and beyond.Amanda is committed to enhancing our understanding of stress, adversity, and trauma while providing tools for personal restoration and growth. By blending extensive training with compassionate, evidence-based practices, she tailors her approach to each individual's or group's unique journey.In our sessions we covered:* What to do during in the margins of our day to regulate our nervous systems and feel rested* How to stop anxiety spiralling at night and get back to sleep (a huge one with neurodivergent sleep challenges combined with menopausal insomnia)* How to manage chronic pain flares and reduce recovery times* S.O.S. techniques for de-escalating sudden panic, suicidal ideation and feelings of hopelessnessWe kept each session brief and succinct because we know that your time is precious. Amanda provided lots of regulating techniques to help us feel emotionally safe throughout the turmoil of the neurodivergent menopause transition. Her tone is so soothing and reassuring, and she makes this work achievable rather than aspirational.Here is a sneak preview! 🎥In the meantime, I hope you are managing the current difficulties life keeps throwing at us all, and that you also have an opportunity to take a break. It is beyond frustrating that the less capacity we have to cope, the more issues come up for us! Please know that you aren’t alone in this. I know how tough it can be, and I think you are doing great. Hang in there. 💕Amanda and I discussed suicide safety plans and the importance of keeping a survival kit close by in times of panic and despair. AI has summed this section up, thank goodness, because I can’t remember - and it was only a few days ago (thanks, brain fog):Mindfulness Tools for OverwhelmAmanda discussed the challenges of managing overwhelming situations without proper safety resources, explaining how the brain can become hyper vigilant or fixated on past or future concerns. She described various personal tools people use to ground themselves in the present moment, such as physical sensations or specific activities, and emphasised that finding an effective tool requires personal discovery. Amanda concluded that these tools serve as circuit breakers to help individuals regain focus and presence.Back to my own words…We chatted about the importance of putting safety plans and regulating tools in place for ourselves when we are feeling well, making us better able to cope with our more difficult days. Using our pattern recognition skills, we can all overcome interoception challenges by noticing how our bodies often feel and what repetitive thoughts emerge before a pain flare, panic attack, suicidal ideation episode and so on. Your safety is of utmost importance, which is why I previously recorded this video for you (in the following post). The best time to plan a suicide safety plan is when you are not feeling at your worst, so that you can utilise your cognitive capacity as much as possible to care for your future self. Neurodivergent menopause is insidious and dynamic, and you may become suddenly vulnerable during times of hormonal flux. If watching the video feels too much right now, the audio only version (44 minutes) can be found here:Autism Adapted Suicide Safety PlanReach out for help, and have an Autism Adapted Safety Plan (AASP) in place:The resources are suggestions to help you understand and complete the safety plan for yourself, or to support another person to complete their safety plan.Step 1 - What are my warning signs that I may start to have strong thoughts, feelings or urges to hurt myself and/or end my life? (e.g., reduced enjoyment in a strong interest, change in routine, change in patterns of sleep, eating, mood)Step 2 - What can I do to help distract myself? (e.g., engage in a particular activity or interest, a relaxation technique, or physical activity)Step 3 - People I can contact to ask for help: (e.g., family, friends, mentor, support worker). Remember to note down when people are, or are not, available (e.g., office hours).Step 4 - Professionals or agencies I can contact during a crisis: (e.g., Samaritans, Mind, A & E, Psychiatric Services). Remember to note down when people are, or are not, available (e.g., opening hours).Step 5 - What can I do to make the environment around myself safer? (e.g., throwing away things that could be used to harm yourself)Step 6 - How can other people help support me?How do I communicate distress? (e.g., I shut down, I have a meltdown)What stresses me/makes me unhappy? (e.g., loud noises, being touched, change of plan, too much information)What can help calm me/makes me happy? (e.g., a strong interest, a quiet safe place to calm down, just sitting with me, giving me my own space)How I would like you to communicate with me? (e.g., don’t ask me to look you in the eye, speak softly, use visual supports, use plain English, keep in mind that I may take what you say literally)Who I would like you to contact?Step 7 – Sharing my safety plan: It can be helpful to share your safety plan. This might be with a trusted friend or family member, health care professional, or support worker. Would you like to share your safety plan? Who would you like to share it with?Storing my safety plan: It can be helpful to think about where you will keep your safety plan so that you can easily access it if you need it (e.g., printed out, in my bag, in a ‘crisis box’, on my phone). It might also be useful to think of any prompts that could help you to remember to use your plan (e.g., having a card with the safety planning logo in it in your wallet to remind you that you have a safety plan).Credit: Autism Adapted Safety Plans at Newcastle University. You can download a copy of the autism adapted safety plan with an accompanying resource pack here. The resources are suggestions to help you understand and complete the safety plan for yourself, or to support another person to complete their safety plan.I am busy replying to comments and all your lovely messages when I see them in my notifications, but my aim is to turn off notifications in August. Please be assured that I am not ignoring you if I don't respond when you message me. I just won’t have seen it. I hope you are able to get some rest and down time. I can’t wait to spend September onwards with you again!Cheers,🐈 🐈⬛ 🐈 🐈⬛ 🐈 🐈⬛ 🐈I’m so glad you are here. If you feel seen and heard by my writing, please consider upgrading to a paid subscription. Paid subscribers support continuous publishing of lived experiences here at The Autistic Perimenopause: A Temporary Regression 💕 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 23m 01s | ||||||
| 7/9/25 |  The Sensory Overload of Menstruation | Hi, I’m Sam Galloway and I have been writing from the nuanced and complex intersection of neurodivergence and menopause for over a year now at The Autistic Perimenopause: A Temporary Regression. I am so glad you are here!Content warning: ectopic pregnancy, abortion, miscarriage, blood, surgery, chronic pain. Every week I forged a sick note for my high school physical education (PE) teacher that said I couldn’t do PE that week, because I was on my period. Every week my PE teacher told me that I needed to learn to get on with it, because I wouldn’t be able to get out of work as an adult just because of my periods. Looking back now I wonder why she didn’t question the frequency of my weekly periods, although we were discouraged from speaking about such matters in my Catholic girls school. The PE communal changing rooms were catty, b****y spaces, where other girls would eye my stretch marks and cellulite, deepening my disordered eating tendencies and low self-esteem. Puberty took me early on. By 11, I was already bleeding, and my weight was double that of my peers. Not curvy, just substantial. Dealing with periods early on in an environment that hushed their presence was difficult. In primary school we received the cursory talk of sex and periods, but it was vague and scant, given the Catholic nature of my education. Emphasis within the curriculum was on theology, with morality based upon being a good girl. In high school, when we were supposedly being taught about contraceptives and birth control, our religious education (RE) teacher played a video about the instruments used to perform an abortion, circa 1995. I don’t know how much detail the video went into the procedure, because one by one every girl ran out of the classroom upset. Being highly sensitive, I was the first to leave, hysterically crying and feeling distraught at the images conjured by my own imagination.Second to leave was my 14 year old classmate and close friend, who had confided in me that she had just had a miscarriage. Her boyfriend was 26. What was their intention in showing us that video? To scare us into not having sex for fear of needing to terminate an unwanted pregnancy? Was it legitimately part of the Catholic RE syllabus, or just a misjudged error on the part of our teacher, a former convent nun?The desired effect wasn’t achieved, as so many girls left school early to have babies. I still don’t understand why frightening girls off abortion was preferential to teaching us how to use contraceptives, and learning about our reproductive systems. Luckily for me, my childhood house was opposite the local community clinic. On Thursday evenings they had the sexual health clinic, and my more cautious wise teenage friends and I would go regularly for check ups, the pill and free condoms. I was clearly unschooling myself from an early age to look beyond the narrow view presented by my so called education. Even back in high school, my periods always came accompanied with extreme menstrual cramping and lower back pain. My bleeds are still debilitatingly painful. Sometimes I am responsive to pain medication, sometimes not. Heat can help; diaphragmatic breathing; focused muscle relaxation. Managing the pain is one thing. Coping with the bleeding is quite another. Bleeding is not a neutral experience for me. I have tried all within my power to stop experiencing it, both consciously and unconsciously: not taking a “pill free week” when on the contraceptive pill, which elicits a withdrawal bleed (rather than a period resulting from ovulation and no subsequent pregnancy). The contraceptive injection in my late teens; the contraceptive implant in my twenties. Pregnancy, long term breastfeeding in my early thirties. When perimenopause took me by surprise in my mid to late thirties, I tried the Mirena IUD, in response to an extensive bleed that lasted many months. Now, I am in a chemical menopause using hormone blockers. In an effort to block out the sensation of bleeding, over the years I have used tampons to try and plug it up. Menstrual cups somehow alleviated associated period pains, although I never acted on the temptation to feed my collected menses to my rose bush. Now the rose bush is dead and gone, yet my bleeding remains. These days I wear period underwear at all times, as much to deal with unpredictable urinary leaking as much as to manage the constant threat of a sudden flow. Over the last week, old pain patterns have trotted out along with sudden, unexpected bleeding. Only this evening I could feel a trickle and couldn’t tell initially if it was a leak or a flow, although the accompanying severe pelvic pain unsubtly hinted at the prospect of yet another evening bleed, which I have had to face each night this past week. Thick blood oozing out of me and collecting in an unwanted pool is beyond what I can tolerate. The sight of it, the smell, the way it streaks and drips and soaks onto other surfaces is all too much.As a wise, kind friend told me a few days ago, “Your body is doing its best, even though you don’t like what it is doing.” She is right. Something is amiss, and I can only assume this hormonal blip is caused by my adding in an extra pump of oestrogen gel last week to my already high dose, in a bid to stop the hip and shoulder pain that has limited my movement recently. But my body is also exquisitely responsive to my mood, perhaps more so than is my mind at times. Tomorrow will be the first anniversary of my dear old Dad’s death, and it has been playing on my mind. I had a random bleed in the UK a year ago as I sat beside him on his deathbed, and another bleed in March this year when my Mum’s visit to us in Aotearoa New Zealand ended.Upon discussion with my GP, I was advised to anticipate further bleeding episodes should any more emotional events occur. Given the random nature of my bleeds, the intense pain, and my hatred of both random events and pain, I am especially glad to be awaiting a hysterectomy in the not too distant future…I cannot wait to no longer bleed. Anaemia is common for women who bleed heavily, and our iron levels need careful monitoring. The patriarchy likes its women too fatigued to put up a fight, so please do us all a favour and keep your iron levels within the normal ranges. Weakness from blood and subsequent iron loss makes me feel dizzy and dissociative, so I tend to eat a steak when I have bled to replace lost iron stores. I also conserve my energy by having a warm Epsom salts bath, then wrapping up in my dressing gown in order to complain endlessly about how much I detest bleeding.Pregnancy losses have been a feature of my adult life, having experienced an ectopic pregnancy and two miscarriages. Our bleeding patterns can communicate to us, if we are receptive to them. Which I am not; I am just reactive to and avoidant of them. Fortunately, when I was bleeding a long streaky prune juice coloured flow, another friend who had experienced an ectopic pregnancy advised me to do a pregnancy test. I was pregnant, but not for much longer, since the ectopic pregnancy was in danger of rupturing and within days I was in emergency surgery. Bleeding in pregnancy was my norm, even with my two out of five successful pregnancies. With my first pregnancy resulting in surgery, I was in constant panic at any sight of blood in my subsequent pregnancies. This week I found out that hypermobility can make bleeding in pregnancy more likely due to tissue fragility and potential clotting problems. Perhaps it is just as well I didn’t have that on the brain at the time.If only we were all prepared for menstruation, and allowed to feel empowered by our bleeds, not shamed for them. Red School is an organisation I wish I had known about decades ago. It feels too late now, my bleeds instill me with a sense of fear, not a sense of power…Imagine that knowledge of the full spectrum and power of the menstrual cycle is commonplace, and we all feel the utter rightness of having this experience within us. Imagine a world in which the menstrual cycle is respected as our spiritual practice. Imagine young people growing up in this menstrual-affirming world.Imagine a world in which menopause is recognized as a healthy, organic step in one's evolutionary journey stepping into the vital and powerful role of serving your community and the world. Imagine knowing that you’ll be profoundly met in the dignity and power of this new place you stand in post menopause.May we all trust our menstrual cycle and reclaim the spiritual significance of Menopause as the path to instate our full sovereignty. May we all recognise and relish our entitlement, dignity and authority to be channels for Menstruality and the Divine Feminine on the planet.Red SchoolI hope that, if are still cycling, you perceive your bleeds from a more holistic perspective than I have ever managed to muster. Looking back, had I learned from Red School, or any indigenous matriarchal culture, that my periods are sacred and healthful, not dirty and shameful, perhaps my pain perception would not be so debilitating. Maybe I wouldn’t actively want them to stop permanently and prematurely, had they not been something to be hushed and hidden in my Catholic school years and beyond. Perhaps I should soak my menses into the garden while I still can, and stand in my power in a bid to relish my entitlement, dignity and authority to be a channel for Menstruality and the Divine Feminine on the planet. Not long after the end of my high school years, my PE teacher was rumoured to have eloped with my Maths teacher, both of them married with families of their own. This was at a time when Catholicism and lesbianism were mutually exclusive. So I am glad that they managed to buck the good girl Catholic trend by midlife. I hope in doing so they reclaimed the spiritual significance of Menopause as the path to instate their full sovereignty. They are certainly better role models, acting on their previously covert love, than our RE teacher was in her overt abortion class. Thanks for reading The Autistic Perimenopause: A Temporary Regression. Paid subscribers make this work possible. 💕🐈 Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 12m 22s | ||||||
| 6/15/25 |  Urinary Incontinence in Perimenopause and Beyond | How has this happened?Birthing two big babies vaginally over a decade ago has finally backfired on me. It’s been a slow burn, with bumps along the path that have led me to a diagnosis of mixed urinary incontinence. It shouldn’t come as too much of a surprise because I experienced extreme fecal urgency shortly after having my first son. He was born weighing a mighty 9lbs 6oz, and required an episiotomy, where the doctor took a pair of scissors to my perineum to dislodge him from my birth canal. I had begged them not to. Being a hyper independent woman, I wanted to “do it alone”, which I could have done, had the maternity staff not insisted on relocating me when I was already in transition from a pool for labouring mothers into a stark clinical birthing room. Their interference stalled my progress, leading to me feeling emotionally unsafe. Repeatedly I asked them if I had pooed myself yet, since I had learnt during antenatal classes that this was a natural sign that the baby’s birth was progressing. I had wanted to poo myself, but they misread this repetitive question for paranoia, anxiety, or something else that I should not have been made to feel in my vulnerable state. Everything slowed down to almost a standstill, and I ended up being instructed to lay flat on my back, feet in stirrups being told to “Push him out of your bottom!” Really it was all a recipe for fecal incontinence, and I have done well to recover especially considering that my GP at the time dismissed this as normal. Baby two born three years later was even heavier at 9lbs 12oz. I water-birthed him at home as an active resistance to unnecessarily over-medicalising his birth. This time around I tore, and stitches healed well after both births. My youngest was almost born in the downstairs toilet, as I was able to completely relax my pelvic floor muscles whilst sitting there, and felt the most comfort in a very uncomfortable situation. What is wrong with me now?Vaginal childbirth is often a contributing factor to later developing bladder incontinence, which seems to be the case for me. Leaking urine didn't really start until my kids became enthusiastic about playing on trampolines, and I wanted to get involved. Going for a wee right before a bounce was not enough to prevent me weeing again immediately mid-bounce. That was a few years ago, and I now know to stay well away from trampolines. My avoidance served me well again for a while, but very recently the leaking has become regular and with less obvious reason. I tried ignoring it and hoping it would just stop. It didn't. So I tried wearing period undies and thinking I could get away with it. Because everyone complains about leaking sometimes, right? A sneeze or a cough can be a common and seemingly unavoidable trigger. Besides, my advertising algorithm is now full of curvy, happy midlife women wearing incontinence pads and living their best lives! I thought it was normal and I just had to put up with it. Although my keen sense of smell meant that I would worry that I smelled of urine. It is one thing to know I have this problem without other people knowing about it too! But then the leaking started happening during my twice weekly personal training sessions. I love working with my trainer, and I told her what was going on. I started following the programme she set me to strengthen, and learn to relax, my pelvic floor. Last Friday it got so bad that I was leaking during the training sessions actively intended to stem the flow. What was wrong with me? Reverse lunge, drip. Reverse lunge, drip. Reverse lunge, drip. Luckily that was the same day that I was seeing the gynaecologist to self-advocate for my hysterectomy. The approval granted for the surgery was a huge weight off my mind, yet the weight of my burgeoning bladder persisted. The gynaecologist internally assessed me and diagnosed a stage one pelvic organ prolapse.Finally, I had an acceptable explanation for my urinary incontinence. It was a medical issue and not a moral failing on my part. I could live with that, and I found it oddly reassuring. All weekend I wondered if the prolapse could soon be repaired surgically during my upcoming hysterectomy. I felt vindicated in my urine leaking pattern - of course I was leaking if I had a prolapse. The prolapse must have occurred whilst birthing my baby boys, and I was asymptomatic until now. But then I worried that the surgery could in fact exacerbate the pelvic organ prolapse, worsening my bladder control. I knew I needed to be proactive in managing this condition, after listening to a great podcast episode on the topic:Why see a pelvic health physiotherapist?Here is a good visual explanation of what the female pelvic floor is and why it matters:Physiotherapist Fiona Rogers talks us through what the pelvic floor is and how it works.Do you know how to do a pelvic floor exercise properly or have you been taught to just suck everything up and in? Watch here how to do it properly.Fiona firmly believes if you understand where the muscles are and how they work then you are more likely to understand and learn how to exercise them properly.Credit: Pelvic Floor ExerciseHormonal changes during menopause can significantly impact the pelvic floor muscles, contributing to symptoms such as urinary incontinence, vaginal wall prolapse, and sexual dysfunction. A pelvic health physiotherapist can assess for muscle weakness, overactivity, or imbalance and develop individualised treatment plans. Interventions may include physiotherapy-guided pelvic floor muscle training, manual therapy, biofeedback, and structured relaxation techniques. These strategies are designed to restore muscular strength, coordination, and neuromuscular control, which supports continence, vaginal wall integrity, and overall pelvic health.Credit: Positive Pelvic Health Already armed with some basic information on my new hyper fixation, I reached out to Jennifer Dutton of Positive Pelvic Health. Jennifer is a pelvic floor physiotherapist who had been highly recommended to me. Amazingly, she offered me a cancellation for an in person initial consultation the very next day. Knowing that verbally retelling my medical issues is overwhelming for me, I brought along the notes I had prepared for the gynaecologist appointment. Jennifer took a very thorough medical background and was empathetic and reassuring. Upon internal examination, both standing and lying down, Jennifer said there was no pelvic organ prolapse present. She explained that vaginas and other organs supported by the pelvic floor will show natural signs of aging in midlife, as our skin loses collagen and oestrogen, also evidenced externally by how our faces, breasts and stomachs may also sag. Here is a video of Jennifer being interviewed about pelvic health, where she explains much of what she told me during my appointment:I wonder if the gynaecologists see any saggy vaginas in their medical training, as mine obviously can’t be a textbook model anymore! With my newly undiagnosed pelvic floor prolapse, I was able to spiral into a new panic about whether indeed my urinary incontinence was just a moral failing on my part after all…What is urinary incontinence?My current issues, known individually as urge incontinence and stress incontinence, together create a combined diagnosis referred to as mixed incontinence. Yay.Urinary incontinence is the unintentional passing of urine. It's a common problem thought to affect millions of people.There are several types of urinary incontinence, including:* stress incontinence – when urine leaks out at times when your bladder is under pressure; for example, when you cough or laugh* urge (urgency) incontinence – when urine leaks as you feel a sudden, intense urge to pee, or soon afterwards* overflow incontinence (chronic urinary retention) – when you're unable to fully empty your bladder, which causes frequent leaking* total incontinence – when your bladder cannot store any urine at all, which causes you to pass urine constantly or have frequent leakingIt's also possible to have a mixture of both stress and urge urinary incontinence.Credit: NHS webpage ‘Urinary Incontinence’.Autism, Interoception and Adult IncontinenceSo I am leaking on the regular, and trying not to blame myself for this recurring issue. It is so normalised yet hidden. TV ads for pads and absorbent pants proliferate, subtly telling us it is okay to leak urine, as long as nobody else knows. Well, f**k that s**t! When I leak, I tell everyone about it. Part of my neurodivergent profile has been a lifelong shamelessness. I don’t feel a need to hide anything. I refuse to feel shame and embarassment for urinary incontinence, despite having a niggling sense of regret that it is happening to me. Urinary incontinence is just another social taboo to stack on top of all the others I make it my mission to bust. Why would being autistic affect my urinary continence? Especially seeing as I am not aware of having any intellectual disability which may be more likely to co-occur with toileting issues. If anything, before perimenopause I may have been considered intellectually gifted. Yet my cognition has declined in this life phase, and I cling to the hope that this regression is temporary and reversible. Interoception is our capacity to identify our internal states and needs. When this is reduced, as mine has been in perimenopause, and is combined with a regression in executive functioning skills, then noticing when I need to use the toilet, and acting on the urge, can lead to me not responding accordingly.Interoception Receptors on our internal organs are responsible for interoception signals that provide information on our internal body and emotional states. Experiences: urge to urinate, hunger, temperature, pain, sadness, joy, anxiety.Interoceptive Over-ResponsivityWith interoception over-responsivity the person feels too much of their internal signals. They “over-feel” their internal sensations. Signs of over-responsivity include:* Visits the nurse’s office several times a week with aches, pains, and illness* Requests frequent bathroom breaks* Limps on an injured knee or ankle for longer than expectedCredit: Dr Megan Anna Neff at Neurodivergent Insights blog post What is Interoception and How to Improve YoursIt seems that my extremely frequent and protracted toilet visits may be down to interoceptive over-responsivity. I have developed an overuse of the toilet that has led to me missing appropriate bodily cues as to when I need to use the bathroom. Unfortunately, this has been the case day and night, and may be a contributing factor to my insomnia. Many of us may have experienced differences in toileting from our neurotypical peers as children, and/or have supported our own neurodivergent children with delayed or fluctuating bladder and bowel control. Neurodivergent people with co-occuring intellectual disabilities may be more likely than those without them to face toileting differences through adolescence and adulthood.I had never anticipated making what I consider in myself to be significant self-care regressions in perimenopause and now continuing into my hormone blocker induced medical menopause. Nobody had ever talked to me about urinary incontinence, as it is such a taboo topic. Until it became an issue in my daily life, it wasn’t forefront of my mind. Yet it would seem that the menopause transition, like during puberty, is a time of developmental shifts and changes. In our capitalist patriarchal society (at least where I live), we are told we should be ever evolving upwards. Improving. Making our lives better for ourselves. Regression is culturally unacceptable and often shunned. So there is little wonder why people mask their incontinence as they age, for fear it could be interpreted as a sign of weakness. As I have been writing for over a year now, The Autistic Perimenopause: A Temporary Regression aims to highlight a common perception for many of our neurokin that this life phase characterised by extreme hormonal flux can lead to regressions and changes in our cognition, energy, emotional regulation, sleep, metabolism and so on. If we conceptualise the spectrum that is autism as a state of constant flux through the lifespan within our social communication, energy, interests, sensory regulation etc. where we can dynamically change in capacity from day to day, or hour to hour, then perhaps it would stand to reason that our interoception and even urinary continence can oscillate over time. It seems from a quick online search that my anti-anxiety medication, Setraline, has urinary incontinence as a known side effect. I started to take it when first diagnosed autistic and highly anxious, as I was unwittingly entering perimenopause, and my kids were asking me to use the trampoline with them often. What a perfect storm! 💦Progesterone intolerance may also be contributing to my urinary incontinence. I have to take progesterone alongside oestrogen in my HRT regimen until I have a total hysterectomy, because progesterone mitigates the potential cancer risk of taking oestrogen. Not only is my progesterone intolerance causing bloating, depression, suicidal ideation at times, but now it may also be counteracting the potential benefits of oestrogen on maintaining my urinary continence. Menopause and IncontinenceThe scale of female urinary incontinence is extreme yet it remains a taboo topic. According to Liz Earle, it takes women 12 years on average of experiencing urinary incontinence symptoms before feeling able to talk to their family doctor. It then takes another two years before they decide to book a doctor’s appointment. Then for many women, their symptoms are dismissed by their doctor. Liz Earle interviewed uroligist (bladder specialist) Dr Vik Khuller on the impact of bladder issues, and he said that “Women suffer in silence… But don’t have to put up with it.” Dr Khuller also discussed the prevalence of bladder and pelvic organ issues in women who have joint hypermobility and/or Ehlers Danlos Syndrome. They also discuss mast cell activation syndrome (MCAS) and “Covid bladder” in this succinct and informative podcast episode:Urinary symptoms are part of the umbrella term genitourinary syndrome of the menopause (GSM), when it occurs due to fluctuating and declining oestrogen levels in perimenopause and beyond.Vaginal oestrogen creams and pessaries can be prescribed to add localised oestrogen back into the area. It is a good option for people who can’t or don’t want to take systemic HRT. It can improve bladder symptoms, vaginal atrophy, vaginal dryness and reduce occurences of urinary tract infections. The Australasian Menopause Society provide further and in depth information in the information booklet entitled, Genitourinary Syndrome of Menopause.Here is an article I wrote last year about vaginal atrophy:What to do if you are experiencing incontinenceIn Menopause and Urinary Incontinence, Healthline advise, “You don’t have to accept occasional bladder leakage as another side effect of menopause or aging. In many cases, there are things you can do to stop and even prevent urinary incontinence… Speak with your doctor to learn more about your condition, treatment options, and outlook.”Different treatments are necessary according to what may be causing urinary incontinence in different people. There is no one size fits all treatment plan, but please do not feel embarassed about it. Go and discuss it with your doctor. They will have heard it all before and can make an appropriate referral, and/or advise on the next best steps to help you. However, should you feel your doctor has dismissed you, that you have medical trauma, or are reluctant to discuss this with your family doctor, perhaps your first step could be to speak to a local pelvic health physiotherapist. In addition, you may like to research the topic further at: Bladder and Bowel CommunityInternational Urogynecological AssociationInternational Continence SocietyStrengthening and relaxing the pelvic floor is keyPelvic health physiotherapist Jennifer Dutton said that, as in my case, pelvic organ prolapse is commonly overdiagnosed, and that recent guidelines advise healthcare practitioners not to tell a woman if she has a stage one pelvic organ prolapse. She said it can create unnecessary concern and, rather, women should be supported to follow an appropriate treatment plan, not feel like they have a medical diagnosis that they are unable to improve. Jennifer also told me that many women have urge and stress incontinence due to tension in the pelvic floor, not weakness as we are always led to believe. So when we are told just to keep doing Kegels or pelvic floor strengthening exercises, it can often make matters worse not better. The plan she has created for me is designed to relax the tension in my pelvic floor muscles, and even out overall strength so that the different parts work together rather than against each other.This includes:* full body massage* using a Shakti mat daily* diaphragmatic breathing* foam rolling my upper legs and mid spine* trigger point spiky ball massage for my glutesIn addition, to cut all caffeine as it is a bladder irritant, and to improve my insomnia. This is already having a marked effect only four days in! I had a caffeine withdrawal headache the first day, but no negative effects thereafter. Coincidentally I started taking non-stimulant Clonidine alongside my ADHD stimulant Vyvanse last week in order to help overcome my insomnia, and to reduce my high blood pressure. Alongside cutting caffeine and introducing relaxing lifestyle changes, this should all be helping improve my overall health and wellbeing. I hope! Bladder retraining techniques have also been explained by Jennifer, and these are difficult to manage during the daytime, but at night I am no longer being frequently woken up by my overactive bladder. This is life changing! Bladder trainingBladder training involves changing habits. It means going to the toilet at set times, even when there's no urge to urinate. If the times between urinating increase little by little, the bladder fills more fully. This helps control the urge to urinate.A bladder-training program often follows these basic steps:* Find the pattern. Keep a diary for a few days. Jot down every time you urinate. A health care provider can use this diary to help you make a schedule for bladder training.* Wait longer before urinating. Your bladder diary can tell you how long you wait between urinating. Add on 15 minutes. If you usually urinate every hour, try to wait for an hour and 15 minutes.Little by little, increase the time between trips to the toilet until you can wait 2 to 4 hours between trips. Increasing the time slowly gives the best chance for success.* Stick to the schedule. Once you've made a schedule, do your best to stick to it. Urinate right after waking up in the morning. And urinate each scheduled time even if you have no urge to go.If you have an urge but it's not time to go, try to wait. Distract yourself or use ways to relax, such as deep breathing. If you feel you're going to have an accident, go to the toilet. But then return to the schedule.Don't give up if you don't succeed the first few times. Keep trying. Your control is likely to increase.Credit: Mayo Clinic’s Bladder Control: Lifestyle strategies ease problemsI now have a two hourly timer on my phone and watch, because part of my neurodivergent presentation is a total inability to sense the passing of time. Every two hours during the daytime, my timer reminds me when I can go to the toilet, and not before! I am building up to managing 3-4 hourly trips before I see my physio Jennifer again in around 6 weeks time. Wish me luck! 🤞 ⏱️ 🚽 💧 🙌Cheers, It takes many hours per week to research and write articles for The Autistic Perimenopause: A Temporary Regression. Please consider becoming a paid subscriber to support my advocacy work. Thank you! Get full access to Divergent Menopause at samgallowayaudhd.substack.com/subscribe | 25m 56s | ||||||
Showing 25 of 48
Pitch Fit is a Pro feature
See how bookable this show is for guests, which brands already advertise, the per-episode ad value, and the best-fit guest and sponsor profile. The numbers are blurred on the free plan.
How readily this show books outside guests like you.
How proven this show is for host-read sponsorships.
For Guests
ProFor Advertisers
ProUpgrade to Pro to unlock guest cadence, sponsor categories, fit scores, and per-episode ad value for this show.