Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Total monthly reach
Estimated from 20 chart positions in 20 markets.
By chart position
- 🇺🇸US · Life Sciences#8030K to 100K
- 🇦🇺AU · Life Sciences#9630K to 100K
- 🇬🇧GB · Life Sciences#1645K to 30K
- 🇨🇦CA · Life Sciences#1785K to 30K
- 🇯🇵JP · Life Sciences#5710K to 30K
- Per-Episode Audience
Est. listeners per new episode within ~30 days
49K to 170K🎙 Daily cadence·23 episodes·Last published 2d ago - Monthly Reach
Unique listeners across all episodes (30 days)
163K to 566K🇺🇸18%🇦🇺18%🇬🇧5%+17 more - Active Followers
Loyal subscribers who consistently listen
65K to 226K
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
Recent episodes
EP Edge Journal Watch Issue 26, June 2026: PFA, LAAO, AF Ablation in Heart Failure, Myocarditis Risk and Sinus Node Biology
Jun 22, 2026
27m 42s
EP Edge Journal Watch Issue 25 June 2026: AF Ablation, Left Atrial Appendage Closure, PFA Workflow, ICD Battery Longevity & Device Tradeoffs
Jun 15, 2026
26m 07s
EP Edge Journal Watch Issue 24 June 2026: AF Ablation in Heart Failure, VT Pulsed Field Ablation, Subcutaneous-ICD Shocks, Wearable Expansion, CABG AF, Genetics and GLP-1 Agonists
Jun 8, 2026
26m 21s
Inaugural EP EdgeTM Journal Watch with Heart Rhythm Society: AVANT GUARD, LAA Closure, OCEAN, and the ALONE-AF Cognitive Substudy
Jun 1, 2026
19m 58s
EP Edge™ Journal Watch Issue 23 May 2026: PFA Durability, Posterior Wall Ablation, Outflow Tract PVCs, and Fitness as Substrate Modification
May 25, 2026
29m 47s
Social Links & Contact
Official channels & resources
RSS Feed
Login
| Date | Episode | Description | Length | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 6/22/26 | 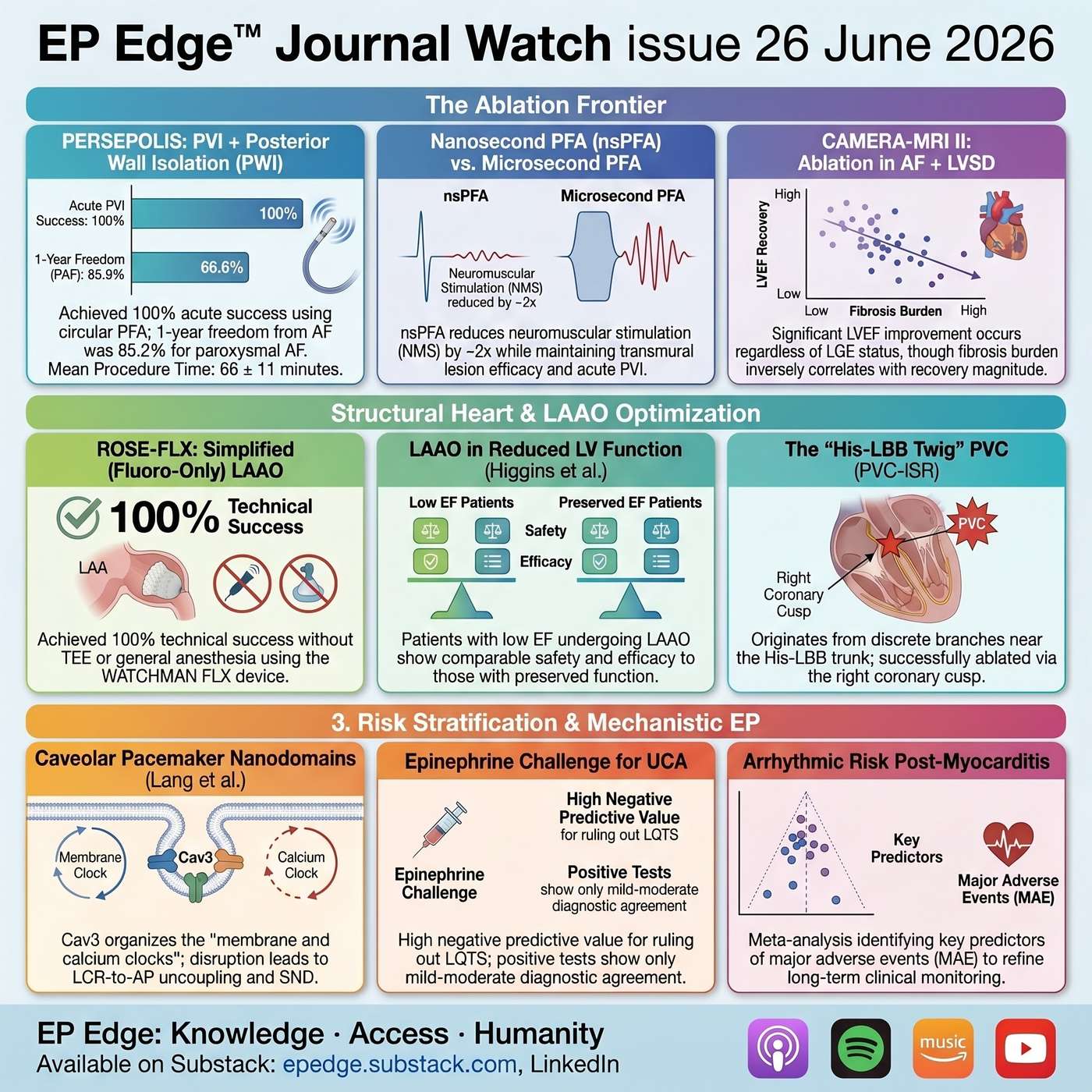 EP Edge Journal Watch Issue 26, June 2026: PFA, LAAO, AF Ablation in Heart Failure, Myocarditis Risk and Sinus Node Biology | In this episode of EP Edge Journal Watch Issue 26, June 2026, Dr. Sharma reviews high-impact studies shaping contemporary cardiac electrophysiology, with a focus on smarter ablation strategies, safer left atrial appendage closure, post-arrest and post-myocarditis risk stratification, and the cellular biology beneath cardiac rhythm.This episode covers pulsed field ablation beyond pulmonary vein isolation, including PVI plus posterior wall isolation in the PERSEPOLIS trial, and nanosecond pulsed field ablation as a potential strategy to reduce neuromuscular stimulation and improve procedural tolerance. Dr. Sharma also reviews catheter ablation for atrial fibrillation with left ventricular systolic dysfunction, focusing on CAMERA-MRI II and what cardiac MRI fibrosis means for recovery, patient selection, and counseling.The episode then moves into left atrial appendage occlusion, including outcomes in patients with reduced ejection fraction and simplified fluoroscopy-guided LAAO workflows. Additional discussions include epinephrine challenge after unexplained cardiac arrest and familial sudden death, the long-term risk of major arrhythmic events after myocarditis, and mechanistic studies on caveolae, pacemaker nanodomains, sinus node dysfunction, and the His-LBB twig as a source of premature ventricular complexes that can look almost identical to sinus rhythm.Rather than simply summarizing abstracts, this episode explains why each study was done, what clinical gap it was designed to address, how the methodology shaped the results, what the statistics mean in practical terms, and how the findings may influence real-world EP decision-making in the lab, clinic, and patient counseling.For full references, graphics, and the written analysis, read EP Edge Journal Watch on LinkedIn and Substack at epedge.substack.com.KeywordsCardiac electrophysiology, EP Edge, EP Edge Journal Watch, Dr. Sharma, electrophysiology podcast, cardiology podcast, heart rhythm, cardiac arrhythmias, atrial fibrillation, AFib, AF ablation, catheter ablation, pulsed field ablation, PFA, nanosecond PFA, pulmonary vein isolation, PVI, posterior wall isolation, PWI, persistent atrial fibrillation, paroxysmal atrial fibrillation, neuromuscular stimulation, AF ablation sedation, left atrial appendage occlusion, LAAO, left atrial appendage closure, reduced ejection fraction, heart failure, HFrEF, LV systolic dysfunction, cardiac MRI, late gadolinium enhancement, LV fibrosis, CAMERA-MRI II, PERSEPOLIS trial, ROSE-FLX, unexplained cardiac arrest, familial sudden death, epinephrine challenge, long QT syndrome, LQTS, CPVT, myocarditis, arrhythmic risk after myocarditis, ventricular arrhythmias, sudden cardiac death, sinus node dysfunction, caveolae, pacemaker nanodomains, His-Purkinje system, PVC ablation, His-LBB twig, premature ventricular complexes, MedEd, CME, cardiology education | 27m 42s | ||||||
| 6/15/26 | 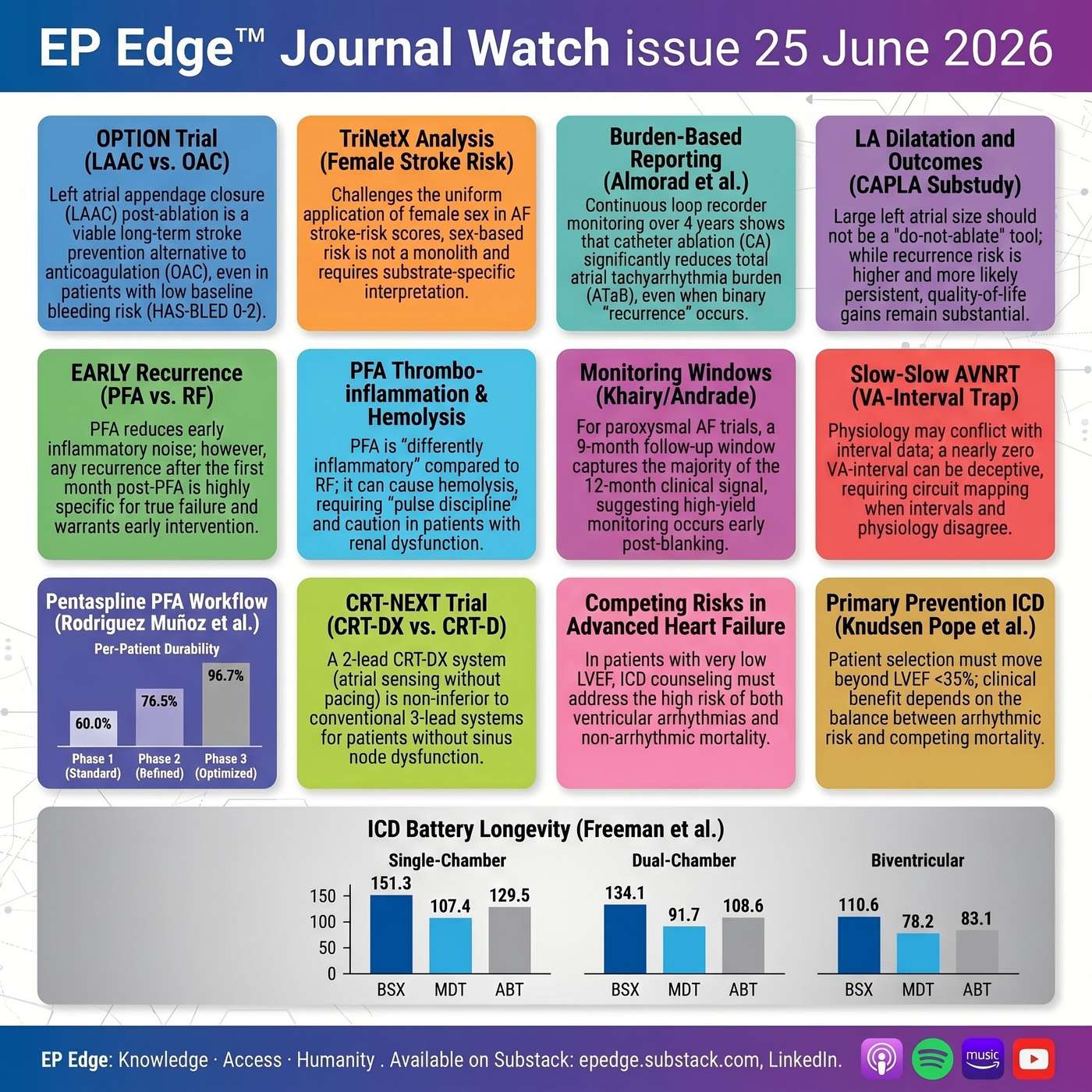 EP Edge Journal Watch Issue 25 June 2026: AF Ablation, Left Atrial Appendage Closure, PFA Workflow, ICD Battery Longevity & Device Tradeoffs | In EP Edge Journal Watch Issue 25, June 2026, Dr. Sharma reviews the most clinically relevant new studies in cardiac electrophysiology, with a focus on atrial fibrillation, stroke prevention, pulsed field ablation, ICD therapy, CRT strategy, and EP lab decision-making.This episode is built around the theme “Beyond the Binary” — moving past simple endpoints like recurrence versus no recurrence, PFA versus RF, EF below 35%, or lead versus no lead. The data in this issue challenge how electrophysiologists think about ablation success, anticoagulation strategy, left atrial appendage closure, device selection, ICD longevity, and arrhythmia risk.Topics covered include:LAAC after AF ablation and the OPTION bleeding-risk substudy: whether left atrial appendage closure after catheter ablation should be considered beyond traditionally high HAS-BLED patients, and how LAAC compares with long-term oral anticoagulation for bleeding reduction and stroke prevention.Female sex and AF stroke risk: a large TriNetX analysis asking whether female sex is truly a uniform stroke-risk factor in atrial fibrillation or better understood as an age- and comorbidity-dependent risk modifier.PFA versus radiofrequency ablation for early recurrence: why pulsed field ablation may reduce symptomatic early recurrence after pulmonary vein isolation, but why early recurrence after PFA still strongly predicts later atrial arrhythmia recurrence.AF burden after ablation: a 4-year continuous-monitoring study showing why binary recurrence endpoints may underestimate meaningful clinical benefit, and why AF burden reduction may be a more patient-centered ablation outcome.Timing of recurrence after paroxysmal AF ablation — pooled trial data suggesting that most post-ablation recurrences are front-loaded, raising important questions about optimal follow-up duration in AF ablation trials.Left atrial size in persistent AF ablation: CAPLA substudy data showing that left atrial volume index may not predict binary recurrence, but may predict recurrence burden and persistent recurrence phenotype.PFA thrombo-inflammation and hemolysis: a detailed look at systemic biological effects after pentaspline PFA, including hemolysis, nitric oxide reduction, renal safety, inflammation, platelet activation, and practical implications for pulse discipline.Optimized pentaspline PFA workflow: systematic remapping data showing that procedural workflow refinement can dramatically improve PVI durability, suggesting that pulmonary vein reconnection may often be a workflow problem rather than a waveform problem.S-ICD therapy in prior monomorphic VT: registry data exploring whether prior monomorphic ventricular tachycardia should automatically exclude patients from subcutaneous ICD therapy, especially when ablation is part of the strategy.CRT-DX versus conventional CRT-D: a randomized noninferiority trial asking whether selected CRT candidates without sinus node dysfunction truly need a dedicated atrial lead.ICD battery longevity by manufacturer, lead burden, and programming: a major device-management study showing clinically meaningful differences in battery longevity across ICD types and manufacturers, including how lead count, programmed output, and pulse width may affect generator replacement risk and lifetime cost.Competing risk in primary prevention ICD therapy: pooled MADIT and RAID data showing that very low LVEF is associated with both higher VT/VF risk and higher competing mortality, refining how clinicians should discuss ICD benefit in advanced heart failure.The nearly zero VA-interval trap: an EP lab pearl on slow-slow AVNRT with prolonged lower common pathway conduction, and why a near-zero VA interval can mimic typical AVNRT.Listen for a practical, clinically focused discussion of how these studies may influence AF ablation follow-up, LAAC selection, PFA workflow, ICD and CRT device choice, sudden death prevention, and EP lab diagnosis.EP Edge Journal Watch is also available as a LinkedIn newsletter and on Substack at epedge.substack.com. References, graphics, and links to the full newsletter are available there.Questions, suggestions, or concerns: epedge.cast@gmail.comKeywords: cardiac electrophysiology, EP Edge Journal Watch, atrial fibrillation, AF ablation, pulsed field ablation, PFA, radiofrequency ablation, pulmonary vein isolation, PVI, left atrial appendage closure, LAAC, OPTION trial, WATCHMAN FLX, AF burden, ICD battery longevity, implantable cardioverter defibrillator, S-ICD, CRT-DX, cardiac resynchronization therapy, ventricular tachycardia, sudden cardiac death, AVNRT, Heart Rhythm, electrophysiology podcast, cardiology podcast. | 26m 07s | ||||||
| 6/8/26 | 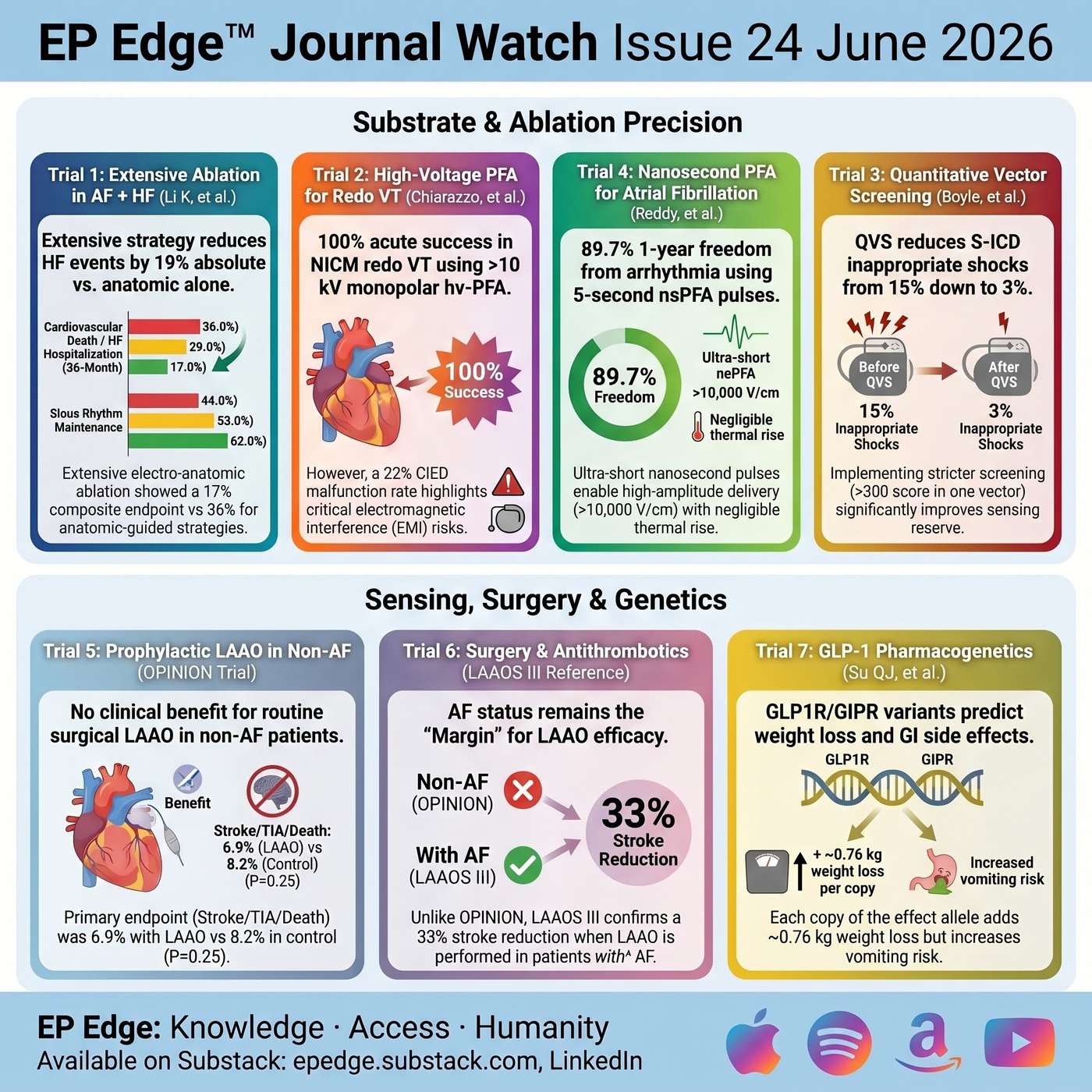 EP Edge Journal Watch Issue 24 June 2026: AF Ablation in Heart Failure, VT Pulsed Field Ablation, Subcutaneous-ICD Shocks, Wearable Expansion, CABG AF, Genetics and GLP-1 Agonists | In this episode of EP Edge Journal Watch, Dr. Sharma reviews major electrophysiology and cardiology studies from Issue 24: Substrate, Sensing, Wearables, Surgery, and the Precision Turn. The central theme is precision EP: selecting the right patient, targeting the right substrate, interpreting the right signal, choosing the right antithrombotic strategy, and designing the right follow-up plan. This episode begins with a randomized trial of persistent atrial fibrillation ablation in patients with heart failure, comparing anatomic-guided ablation, electrogram-guided ablation, and an extensive electrogram-anatomic strategy. The discussion focuses on why pulmonary vein isolation alone may be insufficient in selected patients with persistent AF, atrial myopathy, and heart failure, and how meaningful AF burden reduction may translate into fewer heart-failure hospitalizations and better functional outcomes.Next, Dr. Sharma reviews early experience with high-voltage pulsed field ablation for redo ventricular tachycardia in nonischemic cardiomyopathy. This paper highlights the promise of deeper lesion formation for intramural VT substrate, while also emphasizing major operational challenges, including electromagnetic interference with ICDs, CRT-Ds, and electroanatomic mapping systems.The device EP section covers quantitative vector screening for subcutaneous ICD implantation. Instead of asking only whether an S-ICD vector “passes,” this study asks whether the patient has enough sensing reserve to reduce inappropriate shocks over time. The episode explains how stronger pre-implant vector selection may reduce inappropriate shocks, but also exclude some patients from S-ICD candidacy.The wearable technology discussion reviews a European Heart Journal state-of-the-art paper on smartwatch ECGs, PPG alerts, step counts, heart-failure monitoring, cuffless blood pressure, and AI-enabled cardiovascular data interpretation. Dr. Sharma separates actionable wearable ECG data from screening alerts that require confirmation, longitudinal trends that need context, and consumer metrics that should not drive major treatment decisions without clinical validation.The surgical EP section reviews the OPINION trial, which tested prophylactic surgical left atrial appendage occlusion in patients undergoing valvular surgery without known atrial fibrillation. The episode explains why routine appendage closure in non-AF surgical patients did not significantly reduce ischemic stroke, TIA, or cardiovascular death at one year, and why future AF risk should not be confused with established appendage-mediated thromboembolism.The antithrombotic section focuses on the ESC/EACTS clinical consensus statement on antithrombotic therapy after CABG, with special attention to postoperative AF, established AF, oral anticoagulation timing, DOACs versus VKAs, aspirin, DAPT, graft patency, bleeding risk, and avoidance of routine triple therapy. The key practical message: postoperative AF should not be ignored, but every brief episode should not automatically become lifelong anticoagulation.Finally, the EP Edge Off-track segment examines genetic predictors of GLP-1 receptor agonist weight loss and gastrointestinal side effects, including tirzepatide. Although not an EP trial, this topic matters because obesity, diabetes, sleep apnea, HFpEF, atrial remodeling, AF progression, and ablation durability are all part of the same cardiometabolic substrate.This episode is designed for electrophysiologists, cardiologists, fellows, advanced practice clinicians, researchers, and anyone following modern arrhythmia care, AF ablation, VT ablation, device therapy, wearable monitoring, cardiac surgery, anticoagulation, and cardiometabolic risk modification.Keywords: electrophysiology, atrial fibrillation, AF ablation, persistent AF, heart failure, VT ablation, pulsed field ablation, nonischemic cardiomyopathy, subcutaneous ICD, inappropriate shocks, wearable ECG, smartwatch AF detection, left atrial appendage occlusion, OPINION trial, CABG, postoperative AF, anticoagulation, DOAC, antiplatelet therapy, GLP-1, tirzepatide, EP Edge Journal Watch. | 26m 21s | ||||||
| 6/1/26 | 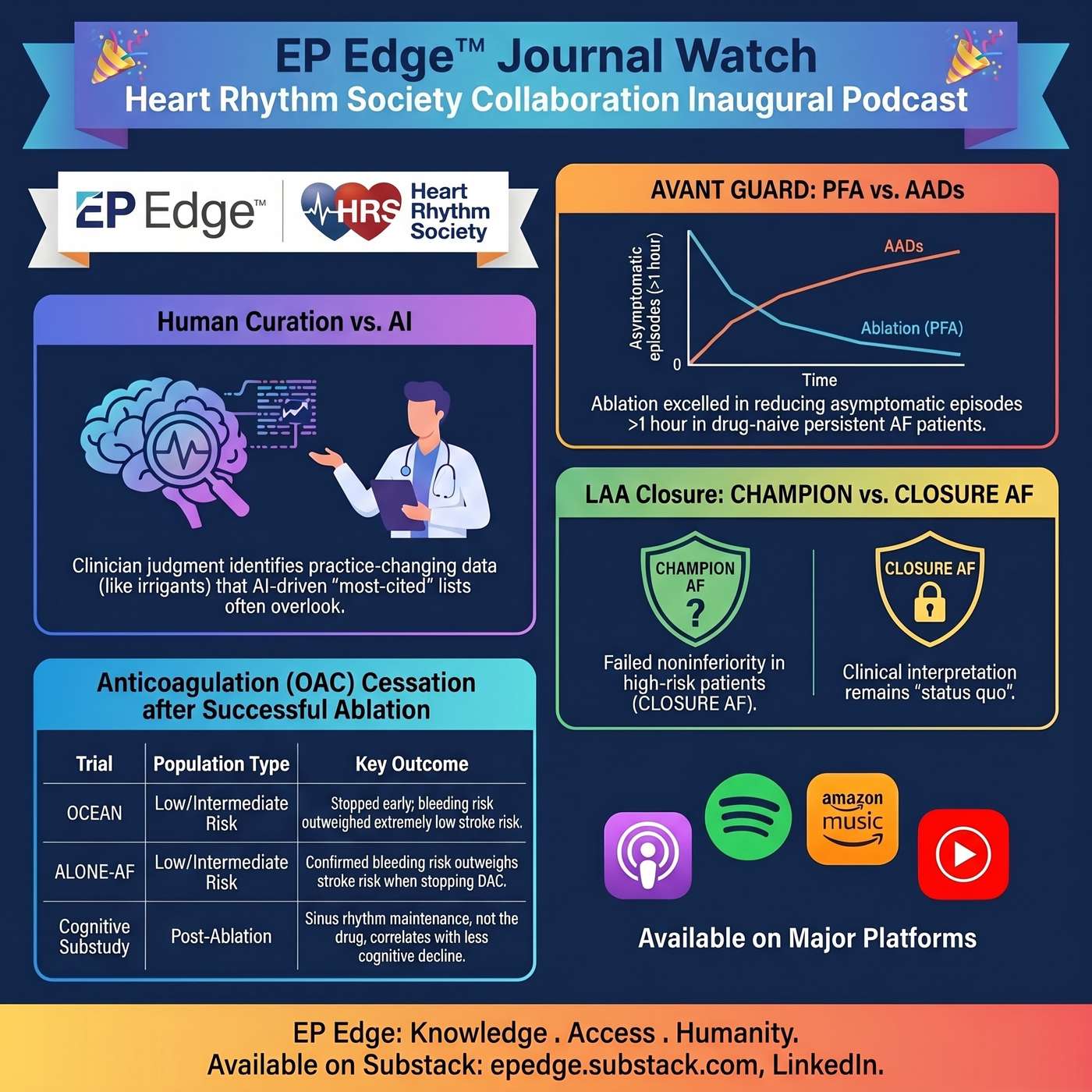 Inaugural EP EdgeTM Journal Watch with Heart Rhythm Society: AVANT GUARD, LAA Closure, OCEAN, and the ALONE-AF Cognitive Substudy | The inaugural EP Edge Journal Watch and Heart Rhythm Society collaboration is here.In this first episode, Dr. Michael Lloyd from the Heart Rhythm Society Digital Education Committee joins Dr. Niraj Sharma, creator of EP Edge, to launch a new monthly format focused on the most clinically relevant literature in cardiac electrophysiology.This is not a routine article summary. It is a practical, physician-led discussion of the studies that matter in the EP lab, in clinic, and at the bedside.Electrophysiology literature is moving quickly. Important trials now appear across major journals, late-breaking sessions, society meetings, and digital platforms. Algorithms can identify highly cited papers. Search tools can rank articles. But clinical relevance still requires judgment. EP Edge Journal Watch was created to help close that gap.The goal is simple: identify the papers that deserve attention, place them in clinical context, and ask what they mean for real patients.In this inaugural episode, Dr. Lloyd and Dr. Sharma begin with AVANT GUARD, a major trial evaluating first-line pulsed field ablation in patients with persistent atrial fibrillation. The discussion goes beyond the headline. They examine patient selection, drug-naive persistent AF, procedural safety, the stroke signal, modified enrollment criteria, anticoagulation requirements, endpoint design, and the difference between symptom reduction and true AF burden reduction.The episode then turns to one of the most active areas in atrial fibrillation care: left atrial appendage closure. Dr. Lloyd and Dr. Sharma discuss CLOSURE AF and CHAMPION AF, two trials that asked similar questions but studied very different patient populations. The discussion focuses on stroke risk, bleeding risk, frailty, procedural complications, endpoint construction, and how these trials should influence shared decision-making. The key clinical question is direct: should left atrial appendage closure be offered broadly as an alternative to anticoagulation, or should it remain focused on patients with a clear problem taking long-term oral anticoagulation?The final section focuses on anticoagulation after apparently successful AF ablation. Dr. Lloyd and Dr. Sharma discuss OCEAN and ALONE-AF, with attention to stroke risk, bleeding risk, patient selection, rhythm monitoring, and the limits of intermittent surveillance. For selected low-risk patients without recurrent atrial arrhythmia, stopping anticoagulation may be reasonable. But the decision is not automatic. It depends on the patient, the risk profile, the quality of rhythm follow-up, and the shared decision-making conversation.The episode also highlights the ALONE-AF cognitive substudy, one of the most interesting parts of the discussion. This substudy moves the conversation beyond stroke and bleeding. It asks whether stopping oral anticoagulation after successful AF ablation affects cognitive function. The key point is nuanced. In selected patients without recurrent atrial arrhythmia, stopping anticoagulation did not appear to produce a cognitive penalty. But the more provocative signal may be rhythm itself. Patients who maintained sinus rhythm appeared to have better cognitive trajectories than those with recurrence.That raises an important clinical question for the field: after AF ablation, is the long-term cognitive story less about the anticoagulant and more about durable rhythm control?This first episode sets the tone for the EP Edge Journal Watch and HRS collaboration. The format is concise, practical, and clinically grounded. It is built for busy electrophysiologists, cardiologists, fellows, advanced practice providers, and clinicians who care for patients with atrial fibrillation.The purpose is not just to summarize trials. It is to interpret them.Which patients were studied?Which endpoints matter?Which findings should change a clinic conversation?Which results should make us pause before changing practice?That is the mission of EP Edge Journal Watch with HRS. | 19m 58s | ||||||
| 5/25/26 | 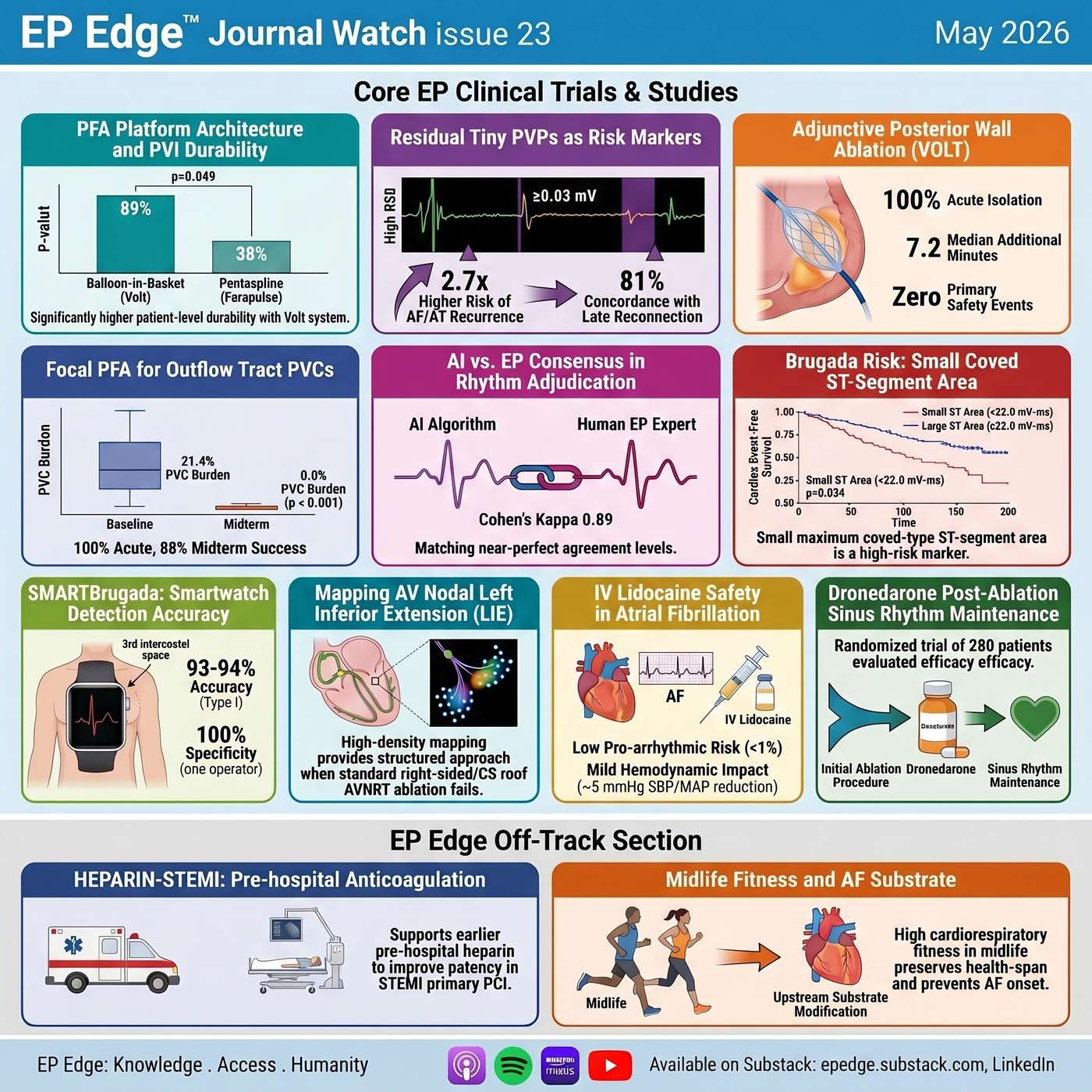 EP Edge™ Journal Watch Issue 23 May 2026: PFA Durability, Posterior Wall Ablation, Outflow Tract PVCs, and Fitness as Substrate Modification | In EP Edge™ Journal Watch Issue 23, May 2026, Dr. Sharma reviews the latest high-impact electrophysiology and cardiology literature with a new focused format: four deep-dive studies and a rapid-fire review of the remaining trials.This episode explores whether pulsed field ablation platform design affects pulmonary vein isolation durability, how balloon-in-basket PFA may change posterior wall ablation, and whether focal PFA is ready for outflow tract PVC ablation. The episode also includes an EP-Edge™ Off-track deep dive on midlife cardiorespiratory fitness and healthy aging, highlighting fitness as upstream cardiovascular substrate modification.Rapid-fire discussions cover residual tiny pulmonary vein potentials after PFA, dronedarone versus amiodarone after AF ablation, AI versus electrophysiologist rhythm adjudication, quantitative Brugada risk stratification, smartwatch detection of Type I Brugada pattern, AV nodal left inferior extension mapping, IV lidocaine safety in AF patients treated for ventricular arrhythmias, and HEPARIN-STEMI.Topics include atrial fibrillation ablation, pulsed field ablation, posterior wall isolation, pulmonary vein durability, PVC ablation, Brugada syndrome, wearable ECG, artificial intelligence in electrophysiology, ventricular arrhythmias, STEMI systems of care, and cardiorespiratory fitness.Full references, graphics, and detailed trial analysis are available in the EP-Edge™ Journal Watch LinkedIn newsletter and on Substack at epedge.substack.com. | 29m 47s | ||||||
| 5/18/26 | 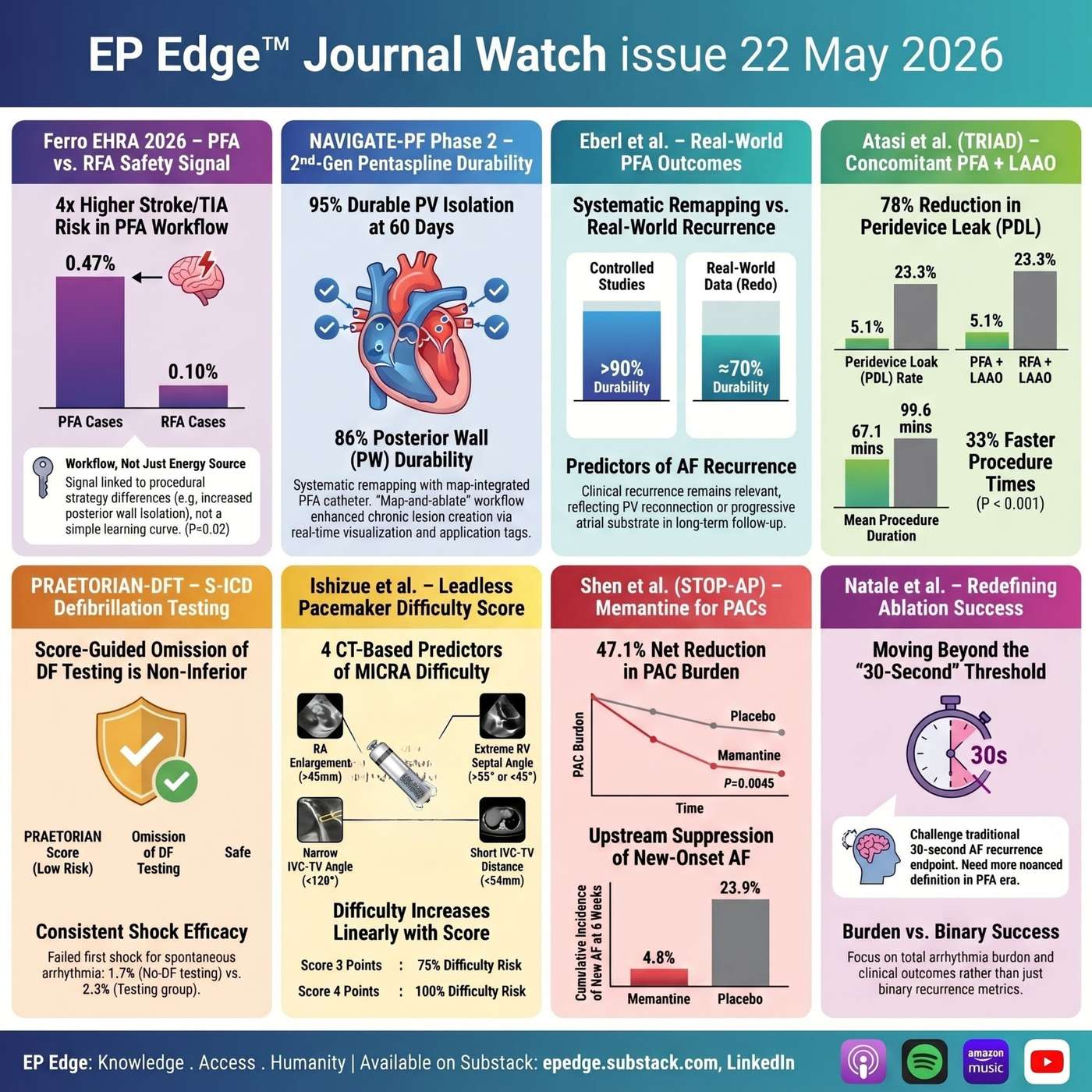 EP Edge Journal Watch Issue 22: PFA Safety, Lesion Durability, LAAO, Subcutaneous-ICD Testing & AF Ablation Success | In this episode of EP Edge® Journal Watch, Dr. Sharma reviews Issue 22, May 2026, focused on the next phase of electrophysiology: pulsed field ablation safety, lesion durability, long-term AF recurrence, one-stop AF procedures, device simplification, PAC suppression, and the evolving definition of ablation success.This issue begins with the Ferro EHRA 2026 real-world comparison of pulsed field ablation versus radiofrequency ablation for atrial fibrillation, highlighting why PFA safety should be interpreted by endpoint, workflow, platform, and lesion strategy rather than as a single global claim.The episode then examines NAVIGATE-PF Phase 2, a systematic remapping study of a second-generation, mapping-integrated pentaspline PFA catheter, and what early lesion durability tells us about the future of anatomically accountable PFA.Dr. Sharma also discusses long-term recurrence after pentaspline PFA, including predictors of AF recurrence and what redo procedures reveal about pulmonary vein reconnection among patients with recurrent arrhythmia.Additional studies include concomitant PFA plus left atrial appendage occlusion, exploring whether a one-stop AF strategy may improve procedural efficiency and reduce peridevice leak; PRAETORIAN-DFT, evaluating whether routine defibrillation testing can be omitted after S-ICD implantation when implant position is favorable; and a CT-based risk score for predicting difficult leadless pacemaker implantation.The episode also covers a provocative phase 2 randomized trial of memantine for premature atrial contractions, introducing NMDA receptor antagonism as a potential nontraditional pathway for atrial ectopy suppression.Finally, this issue closes with a critical look at how we define success after AF ablation. Is the traditional 30-second atrial arrhythmia recurrence endpoint still enough in the PFA era, or should future trials prioritize AF burden, symptoms, repeat procedures, antiarrhythmic drug use, quality of life, healthcare utilization, and safety by domain?This episode is designed for electrophysiologists, cardiologists, EP fellows, APPs, device specialists, and clinicians who want concise, clinically grounded interpretation of the latest EP literature.Full references and graphics are available in EP Edge Journal Watch on LinkedIn and Substack: epedge.substack.com.Questions, concerns and suggestions: epedgecast@gmail.com | 33m 37s | ||||||
| 5/11/26 | 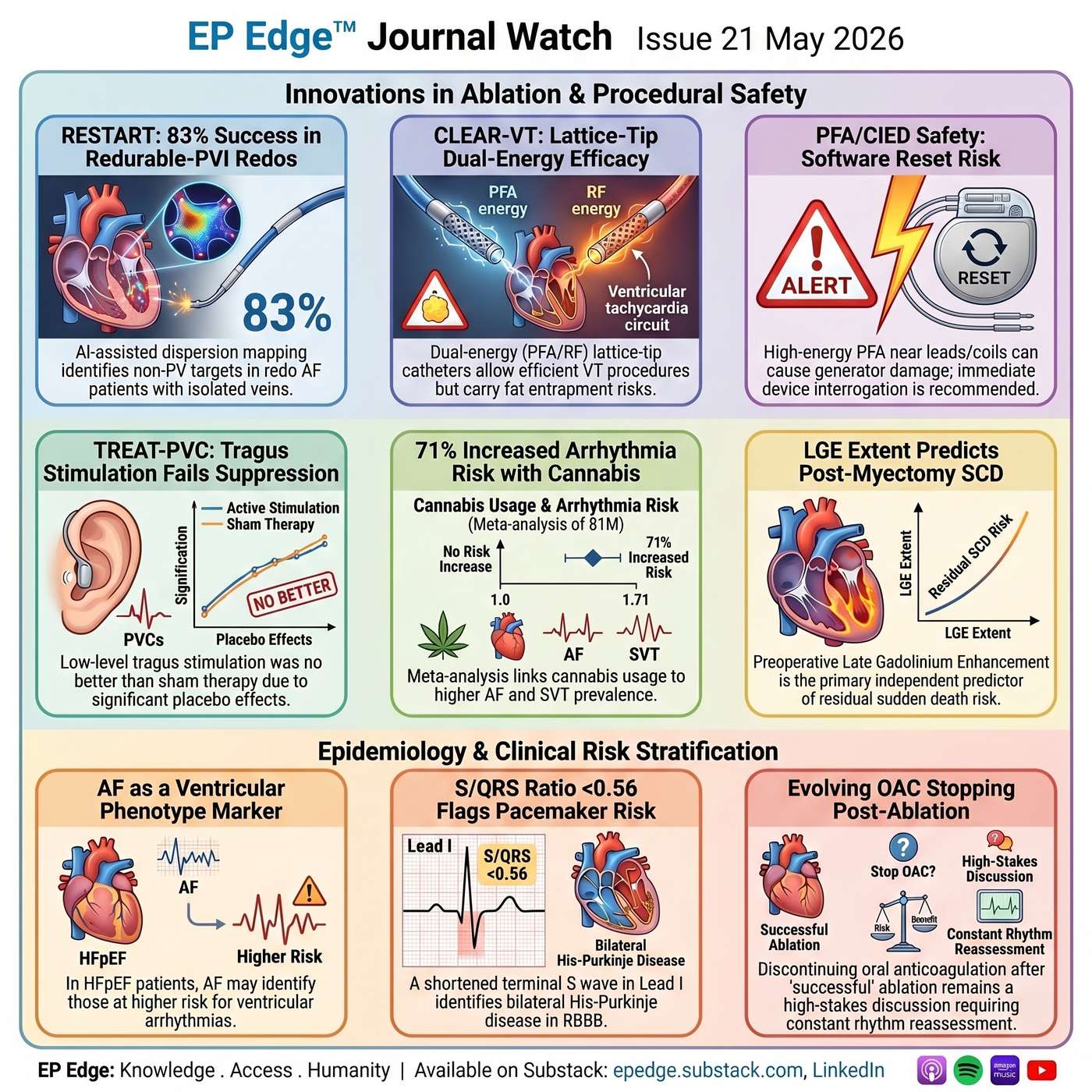 EP Edge™ Journal Watch Issue 21 May 2026: AI-Guided AF Ablation, PFA/CIED Safety, VT Ablation, Cannabis and Arrhythmia Risk, HCM, HFpEF, RBBB, and Anticoagulation After AF Ablation | In this May 2026 episode of EP Edge™ Journal Watch, we review nine high-impact electrophysiology studies shaping contemporary EP practice. This issue covers AI-guided redo AF ablation, dual-energy lattice-tip ventricular arrhythmia ablation, pulsed field ablation safety in patients with cardiac implantable electronic devices, neuromodulation for PVC suppression, cannabis-associated atrial arrhythmia risk, sudden death risk after HCM myectomy, atrial fibrillation as a ventricular arrhythmia risk marker in HFpEF, post-ablation anticoagulation strategies, and a practical ECG marker for pacemaker risk in right bundle branch block.1. RESTART Trial: AI-guided redo AF ablation in patients with isolated pulmonary veins The RESTART trial examines one of the most difficult redo AF scenarios: recurrent symptomatic atrial fibrillation despite durable pulmonary vein isolation. The study evaluates whether AI-guided electrogram dispersion mapping can identify non-PV substrate and guide a more disciplined redo ablation strategy rather than relying on empirical lesion sets.2. CLEAR-VT: Dual-energy lattice-tip ablation for ventricular arrhythmias CLEAR-VT reports early U.S. experience using a dual-energy lattice-tip catheter capable of radiofrequency and pulsed field ablation for complex ventricular arrhythmias. The study is important because it highlights both the promise of broader lesion delivery in scar-related VT and the need for a new safety framework around device interaction, ventricular dosing, and substrate-specific limitations.3. PFA/CIED safety cluster: Device reset, generator damage, VF, and lead-mediated risk This section reviews a group of reports describing clinically relevant interactions between high-energy ablation systems and pacemakers, ICDs, CRT devices, leadless pacemakers, and ICD coils. The key issue is that PFA is tissue selective, but it is still an electrical therapy delivered in patients with conductive hardware, making pre- and post-procedure device interrogation, imaging awareness, and lesion planning essential.4. TREAT-PVC: Transcutaneous vagus nerve stimulation for PVC suppression TREAT-PVC tests whether low-level tragus stimulation can reduce symptomatic idiopathic PVC burden compared with sham stimulation. The central lesson is not simply whether neuromodulation works, but how strongly placebo effects, PVC variability, and potentially active sham physiology can affect device-based autonomic trials.5. Cannabis use and atrial arrhythmias: Systematic review and meta-analysis This large meta-analysis evaluates the association between recreational cannabis use and atrial arrhythmias, including atrial fibrillation, atrial flutter, atrial tachycardia, and SVT. The findings do not prove causality, but they make cannabis clinically relevant in arrhythmia history-taking, especially in younger patients, unexplained palpitations, AF, flutter, or SVT.6. Postmyectomy hypertrophic cardiomyopathy: Residual sudden death risk This CMR-based cohort evaluates predictors of sudden cardiac death after surgical septal myectomy in obstructive HCM. The key clinical message is that myectomy can relieve obstruction, but it does not erase myocardial fibrosis, so late gadolinium enhancement remains important in ICD and surveillance discussions.7. AF in HFpEF: Marker of ventricular tachyarrhythmia or cardiac arrest risk This study explores whether atrial fibrillation in HFpEF identifies patients at higher risk for ventricular tachyarrhythmias or cardiac arrest. It should not be interpreted as an ICD-indication study, but it raises an important hypothesis: AF in HFpEF may be a marker of deeper atrial-ventricular remodeling, fibrosis, autonomic dysfunction, or comorbidity clustering.8. Long-term antithrombotic strategies after AF ablation: Network meta-analysis of randomized trials This analysis addresses one of the most practice-sensitive questions in AF management: whether anticoagulation can be safely stopped after apparently successful AF ablation. The signal is provocative, but the boundary remains narrow because event rates are low and high-risk patients remain underrepresented; this is a shared-decision paper, not a broad permission slip to stop OAC.9. S/QRS ratio in lead I: ECG clue to pacemaker risk in RBBB This study examines whether the S-wave duration in lead I, expressed as a fraction of total QRS duration, can help identify patients with RBBB who may be at higher risk of requiring a pacemaker. The practical takeaway is simple: in RBBB, do not only measure QRS width—look carefully at lead I, because a short terminal S wave may suggest more diffuse His-Purkinje disease.Across all nine studies, the theme is consistent: modern electrophysiology is becoming more powerful, more data-driven, and more device-dependent, but the clinical edge still comes from judgment. EP Edge™ Journal Watch translates these studies into practical EP interpretation for electrophysiologists, cardiologists, EP fellows, APPs, and clinically engaged trainees.The full written issue, graphics, references, and subscription links are available through EP Edge™ Journal Watch on LinkedIn and Substack at epedge.substack.com. | 39m 09s | ||||||
| 5/4/26 | 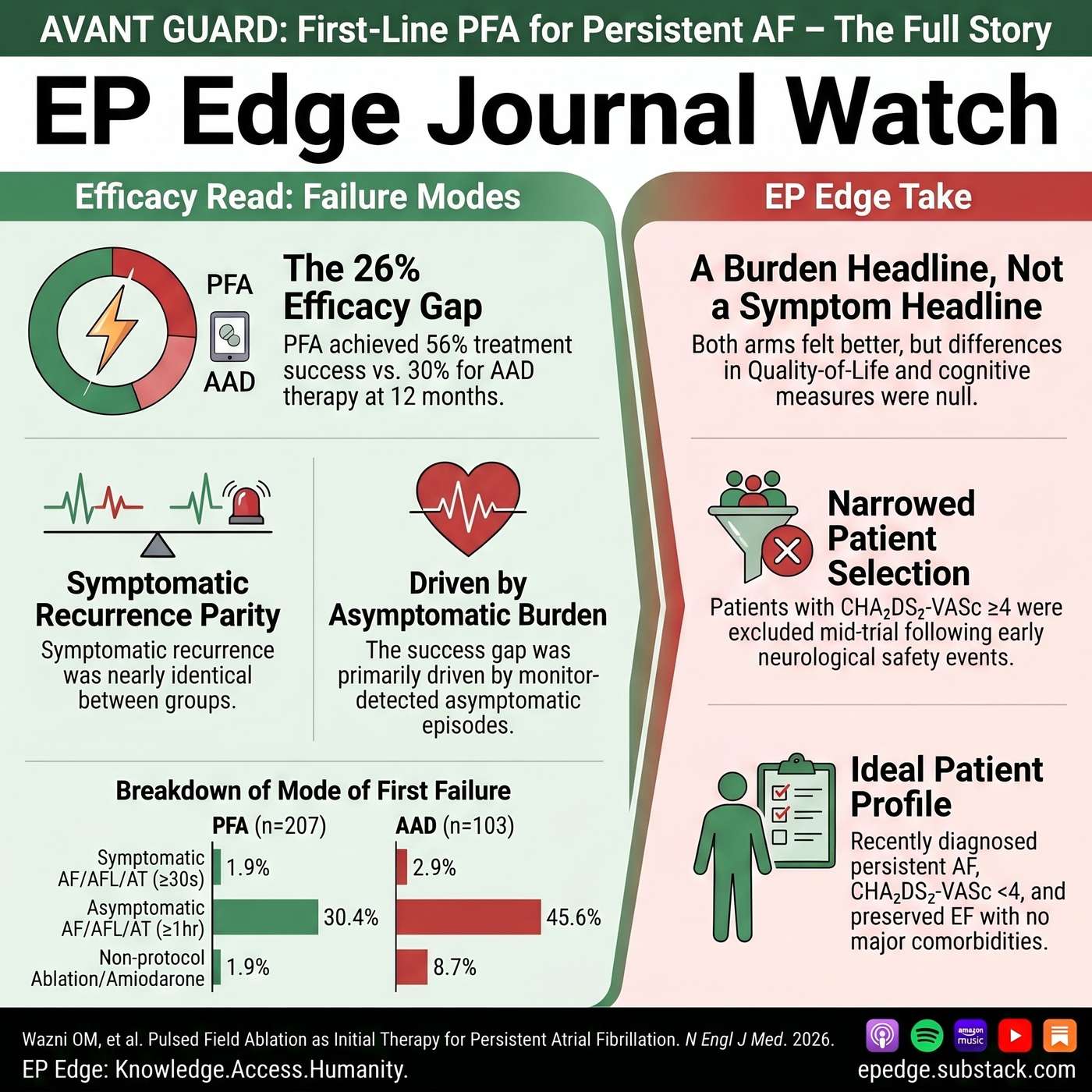 EP Edge™ Journal Watch: AVANT GUARD Trial, PFA as First-Line Therapy for Persistent AF: Half the Story | In this special HRS 2026 edition of EP Edge™ Journal Watch, Dr. Niraj Sharma takes a deep, clinically focused look at the AVANT GUARD trial, published in The New England Journal of Medicine, evaluating pulsed field ablation as initial therapy for treatment-naïve persistent atrial fibrillation.AVANT GUARD delivered the headline many expected: first-line PFA reduced atrial arrhythmia recurrence and AF burden compared with antiarrhythmic drug therapy, with 12-month freedom from atrial arrhythmia of 56% versus 30%. But the story underneath is more complex.This episode examines why AVANT GUARD may influence future AF guidelines while also requiring careful interpretation. Dr. Sharma breaks down the trial design, including the randomized efficacy arm and the separate single-arm safety cohort, the exclusion of amiodarone from the comparator arm, the role of continuous monitoring, and why the primary efficacy result depends heavily on asymptomatic AF detection.The episode also explores the mid-trial safety pause after six neurological events, the post-pause protocol changes, the exclusion of patients with CHA₂DS₂-VASc ≥4, and the unresolved questions around female sex, stroke risk, and generalizability. Quality-of-life outcomes, symptomatic recurrence, adverse events, crossover to ablation, and patient counseling implications are reviewed in detail.Key topics include:Pulsed field ablation, persistent atrial fibrillation, AVANT GUARD trial, FARAPULSE, antiarrhythmic drugs, AF burden, asymptomatic AF recurrence, CHA₂DS₂-VASc, stroke risk, first-line AF ablation, HRS 2026, and electrophysiology trial interpretation.The EP Edge™ take: AVANT GUARD is a positive and important trial, but it is not a simple “PFA works twice as well” story. The trial supports first-line PFA for selected treatment-naïve persistent AF patients, but it does not prove superior symptom relief, quality-of-life improvement, or hard-outcome benefit at 12 months.Full references and graphics are available in the EP Edge Journal Watch LinkedIn newsletter and on Substack at epedge.substack.com | 24m 08s | ||||||
| 4/27/26 | 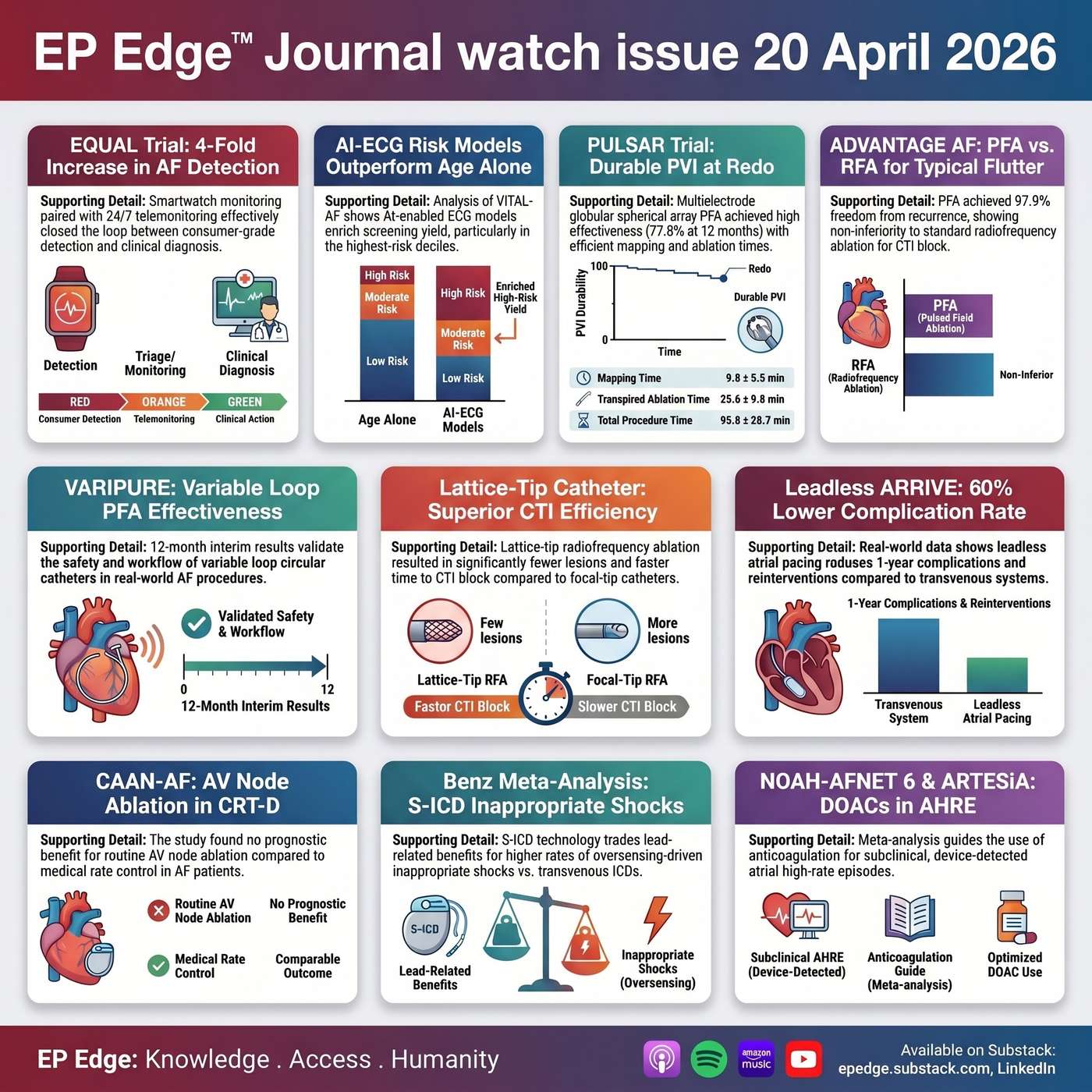 EP Edge™ Journal Watch Issue 20: AF Screening, Pulsed Field Ablation, ICD Shocks, CRT in AF, and Anticoagulation After Ablation | In this episode of EP Edge™ Journal Watch Issue 20, Dr. Sharma reviews some of the most clinically relevant new developments in cardiac electrophysiology, with a sharp focus on atrial fibrillation screening, pulsed field ablation expansion, device therapy trade-offs, and post-ablation anticoagulation strategy.This issue examines how Apple Watch–based atrial fibrillation detection performed in a randomized trial, and whether wearable screening becomes truly useful only when paired with a real adjudication workflow. It also reviews AI-enabled ECG risk models for AF screening, highlighting how precision screening may outperform broad age-based approaches by identifying the patients most likely to benefit from active surveillance.On the device side, this episode analyzes the randomized evidence comparing subcutaneous versus transvenous implantable cardioverter-defibrillators, with special attention to the mechanisms behind inappropriate shocks and how that should influence real-world patient counseling. It also covers the CAAN-AF trial, asking whether atrioventricular node ablation in patients with cardiac resynchronization therapy and permanent atrial fibrillation should remain routine when baseline rate control is already acceptable. In addition, the episode discusses new real-world data on leadless atrial pacing with AVEIR AR versus transvenous pacing for sinus node dysfunction, focusing on complications, reinterventions, and front-line device selection.A major section of the podcast is devoted to the rapid evolution of pulsed field ablation. Dr. Sharma reviews data on PFA versus radiofrequency ablation for typical atrial flutter, the LINEAR randomized trial of lattice-tip versus standard focal-tip catheter ablation for cavotricuspid isthmus lesions, and two important platform-specific studies—PULSAR and VARIPURE—that address lesion durability, workflow efficiency, and the growing question of whether next-generation PFA systems can deliver more reproducible pulmonary vein isolation in contemporary practice.The episode closes with a practical discussion of oral anticoagulant discontinuation after successful AF ablation, examining new data on the timing of anticoagulation withdrawal and the ongoing tension between bleeding reduction and thromboembolic protection.If you follow atrial fibrillation, catheter ablation, implantable cardioverter-defibrillators, cardiac resynchronization therapy, leadless pacing, wearable AF detection, and contemporary electrophysiology trials, this episode is built for you. Expect concise trial summaries, clear statistical interpretation, and the EP Edge™ critical appraisal of what these findings should actually mean for clinical practice.All references and graphics are available through the EP Edge Journal Watch newsletter on LinkedIn as well as on Substack at epedge.substack.com. | 31m 12s | ||||||
| 4/20/26 | 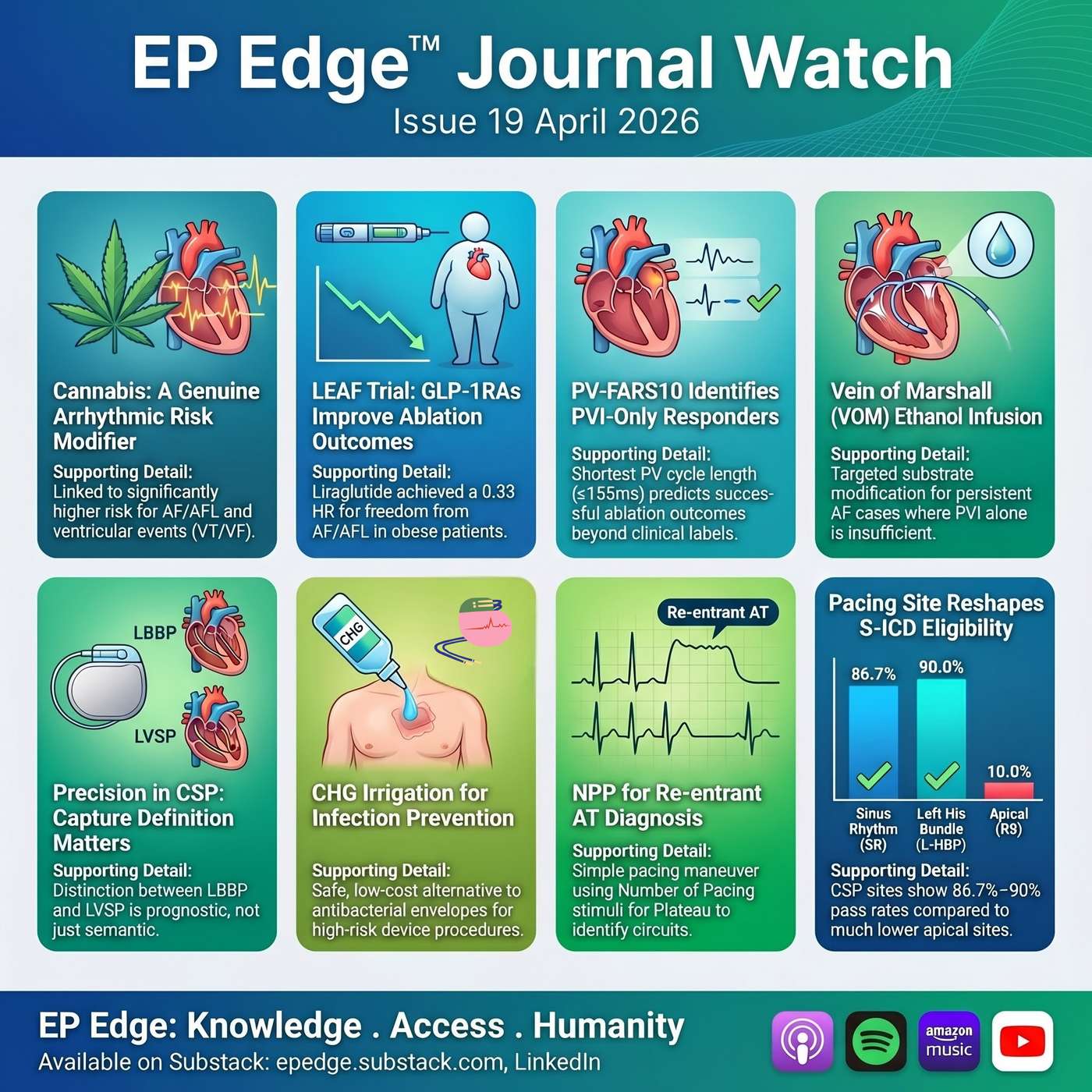 EP Edge™ Journal Watch Issue 19: Atrial Fibrillation Ablation, Conduction System Pacing, GLP-1 Therapy and Arrhythmia Risk | In EP Edge™ Journal Watch Issue 19, Dr. Sharma reviews the most important new studies in atrial fibrillation ablation, conduction system pacing, device therapy, and real-world arrhythmia risk. This episode covers a large multicenter analysis linking cannabis use with higher rates of atrial fibrillation, tachycardia, premature beats, and ventricular arrhythmias; the LEAF study on liraglutide and AF ablation outcomes in overweight and obese patients; and FARS-AF II, which suggests a pulmonary vein physiologic signal may help identify PVI-only responders better than traditional paroxysmal-versus-persistent AF labels.The episode also examines the growing role of vein of Marshall ethanol infusion in persistent atrial fibrillation, the ChiCSP study on long-term outcomes with His bundle pacing, left bundle branch pacing, and left ventricular septal pacing, and a practical paper showing how pacing site can affect subcutaneous ICD screening eligibility. Additional highlights include a device infection prevention study comparing chlorhexidine pocket irrigation versus antibacterial envelope use in high-risk CIED procedures, and a novel EP maneuver using NPP, or the number of pacing stimuli needed to attain a plateau post-pacing interval, to help define proximity to a re-entrant atrial tachycardia circuit.This is a high-yield episode for electrophysiologists, cardiologists, fellows, nurse practitioners, physician assistants, nurses, and allied EP professionals who want a clinically focused review of the latest data in AF ablation, conduction system pacing, S-ICD strategy, CIED infection prevention, and cardiac electrophysiology practice.A shorter, slightly punchier title option would be:EP Edge™ Journal Watch Issue 19: AF Ablation, Conduction System Pacing, GLP-1 Therapy, S-ICD Strategy and Arrhythmia RiskThis title and description are built around the Issue 19 paper set, including the cannabis-arrhythmia analysis, LEAF, FARS-AF II, the vein of Marshall review, ChiCSP, the S-ICD pacing-site paper, CHG versus antibacterial envelope, and the NPP study.All details of these trials including references illustrations are available on the EP edge Journal watch newsletter available on LinkedIn as well as substack: epedge.substack.com | 18m 04s | ||||||
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 4/14/26 | 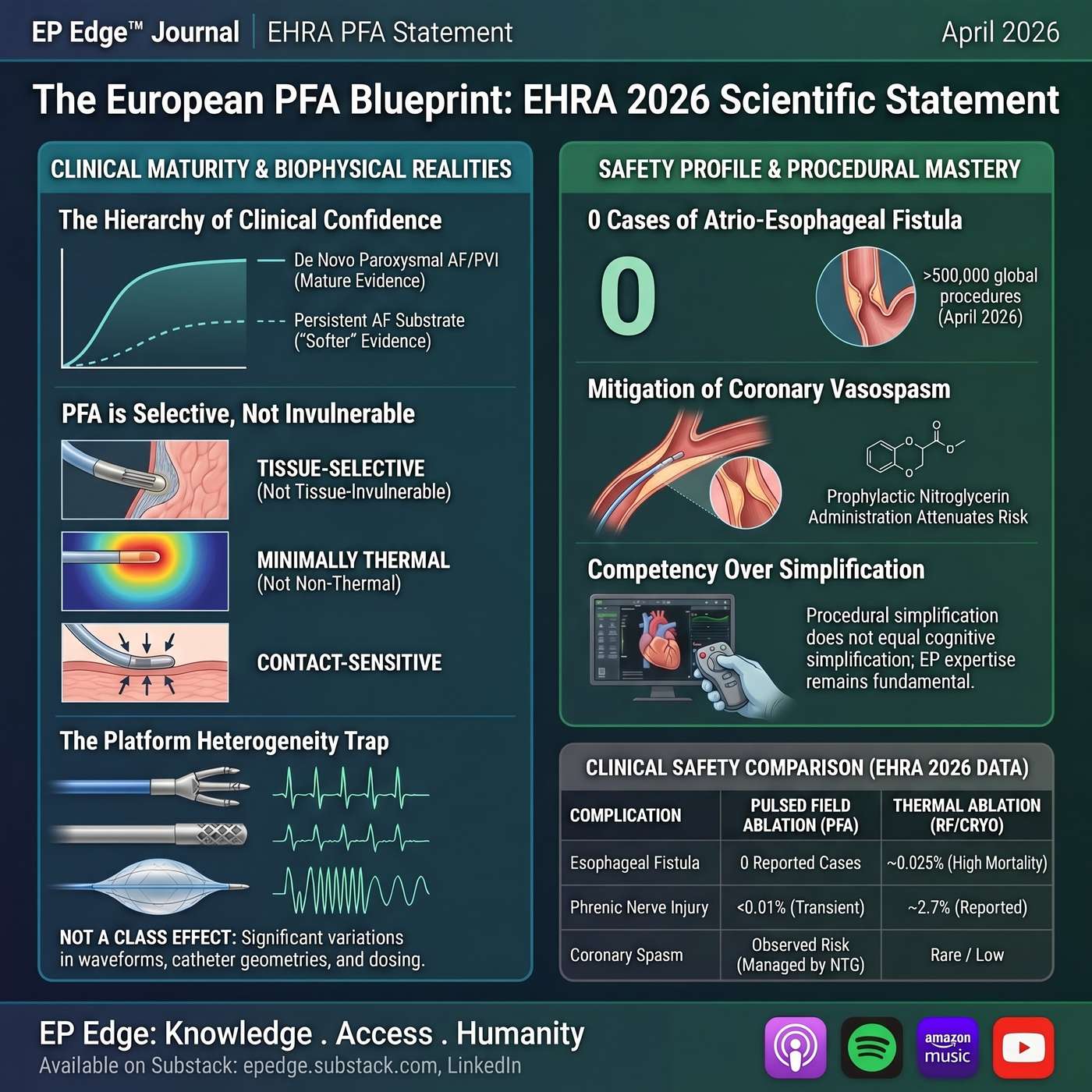 EP Edge™ Journal Watch Special Edition: EHRA PFA Statement 2026 | What the New Guidance Means for AF Ablation | In this special edition of EP Edge™ Journal Watch, Dr. Sharma takes a focused, critical look at the 2026 EHRA/ESC scientific statement on pulsed field ablation for atrial fibrillation. This episode goes beyond a surface summary to examine what the new EHRA PFA statement adds to the field, where it is most useful in day-to-day electrophysiology practice, and where important evidence gaps still remain.The discussion reviews the statement’s key themes, including PFA biophysics, platform heterogeneity, patient selection, procedural workflow, safety, training, and emerging applications. It also compares the EHRA statement with the 2026 HRS scientific statement, highlighting where the two documents align and where EHRA offers a broader, more practical, and more workflow-oriented perspective.For electrophysiologists, trainees, and anyone following the rapid evolution of pulsed field ablation in atrial fibrillation, this episode provides a concise but rigorous overview of what this new document means for contemporary AF ablation practice.All references are available on the LinkedIn EP Edge Journal Watch newsletter, as well as on Substack at epedge.substack.com | 21m 43s | ||||||
| 4/13/26 | 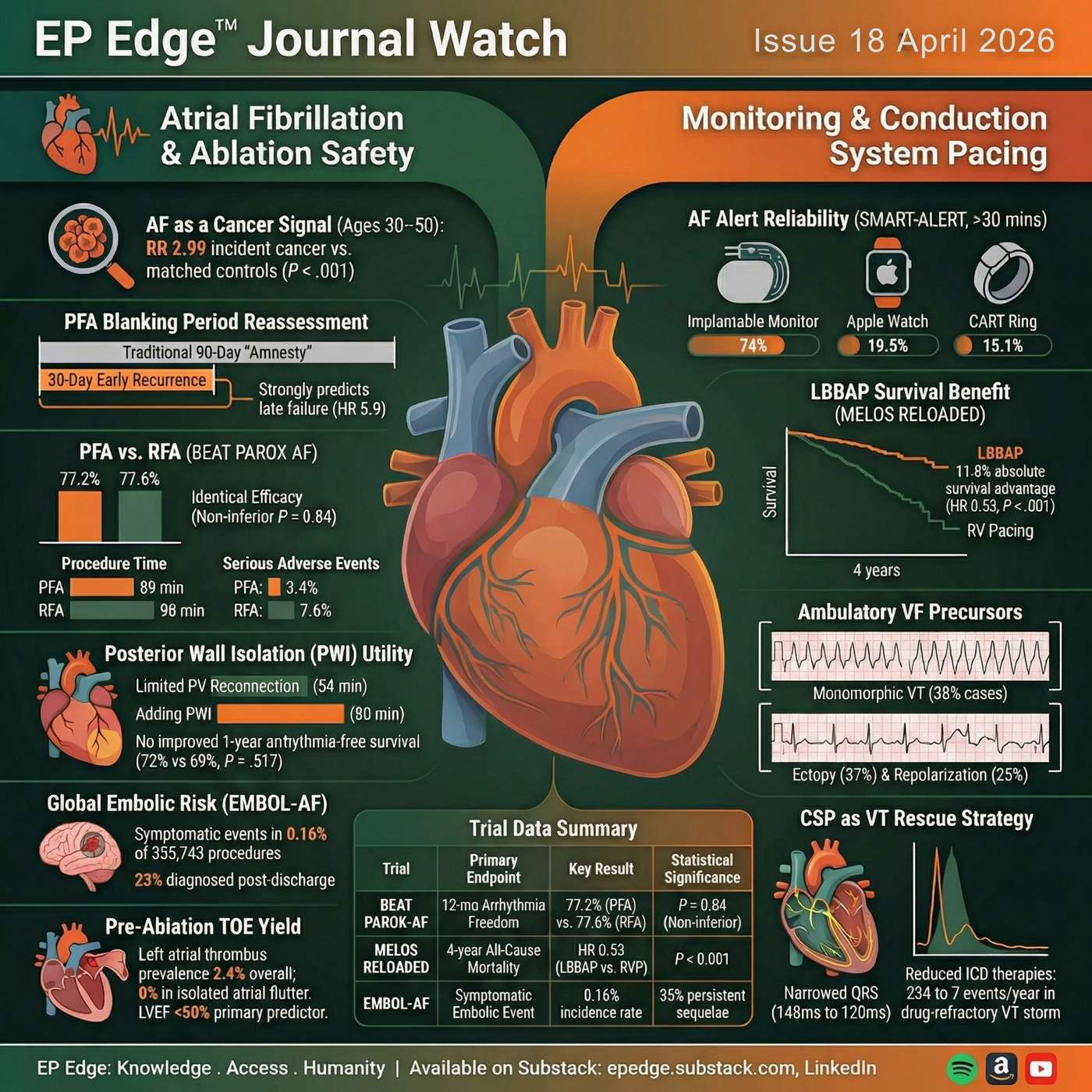 EP Edge™ Journal Watch Issue 18 (April 2026): AF Cancer Signals, PFA Recalibration, EMBOL-AF, SMART-ALERT, LBBAP, and VT Rescue | In EP Edge™ Journal Watch Issue 19 (April 2026), Dr. Niraj Sharma takes a high-level look at the latest developments in cardiac electrophysiology, with a sharp focus on atrial fibrillation, pulsed field ablation, embolic risk, physiologic pacing, and ventricular arrhythmia rescue strategies.This episode moves beyond routine rhythm-control discussions and examines whether new-onset atrial fibrillation may serve as a marker of incident cancer, why the traditional 90-day blanking period after AF ablation may need reassessment in the era of pulsed field ablation (PFA), and what the BEAT PAROX-AF trial actually showed when PFA was tested head-to-head against optimized radiofrequency ablation. The episode also reviews whether posterior wall isolation adds value during redo AF ablation, and analyzes the EMBOL-AF Global Registry, which offers one of the most important contemporary looks at stroke and systemic embolism after atrial fibrillation ablation. Additional discussions include a selective approach to left atrial thrombus imaging before ablation, the SMART-ALERT study on real-time smartphone notifications for AF episodes, long-term outcome data comparing left bundle branch area pacing with right ventricular pacing in atrioventricular block, novel ambulatory precursors of ventricular fibrillation, and an intriguing small series exploring conduction system pacing as an alternative or bridging strategy in drug-refractory ventricular tachycardia. This podcast is designed for electrophysiologists, cardiologists, fellows, advanced practice providers, researchers, and the broader EP community looking for concise but rigorous analysis of the most clinically meaningful new studies in arrhythmia care. Expect expert discussion of AF ablation, PFA trials, stroke prevention, left bundle branch pacing, ventricular tachycardia, and the evolving science shaping modern EP practice. All references and details are available on the LinkedIn newsletter as well as on Substack, epedge.substack.com. Any questions, concerns, or suggestions can be sent to epedgecast@gmail.com | 29m 49s | ||||||
| 4/6/26 | 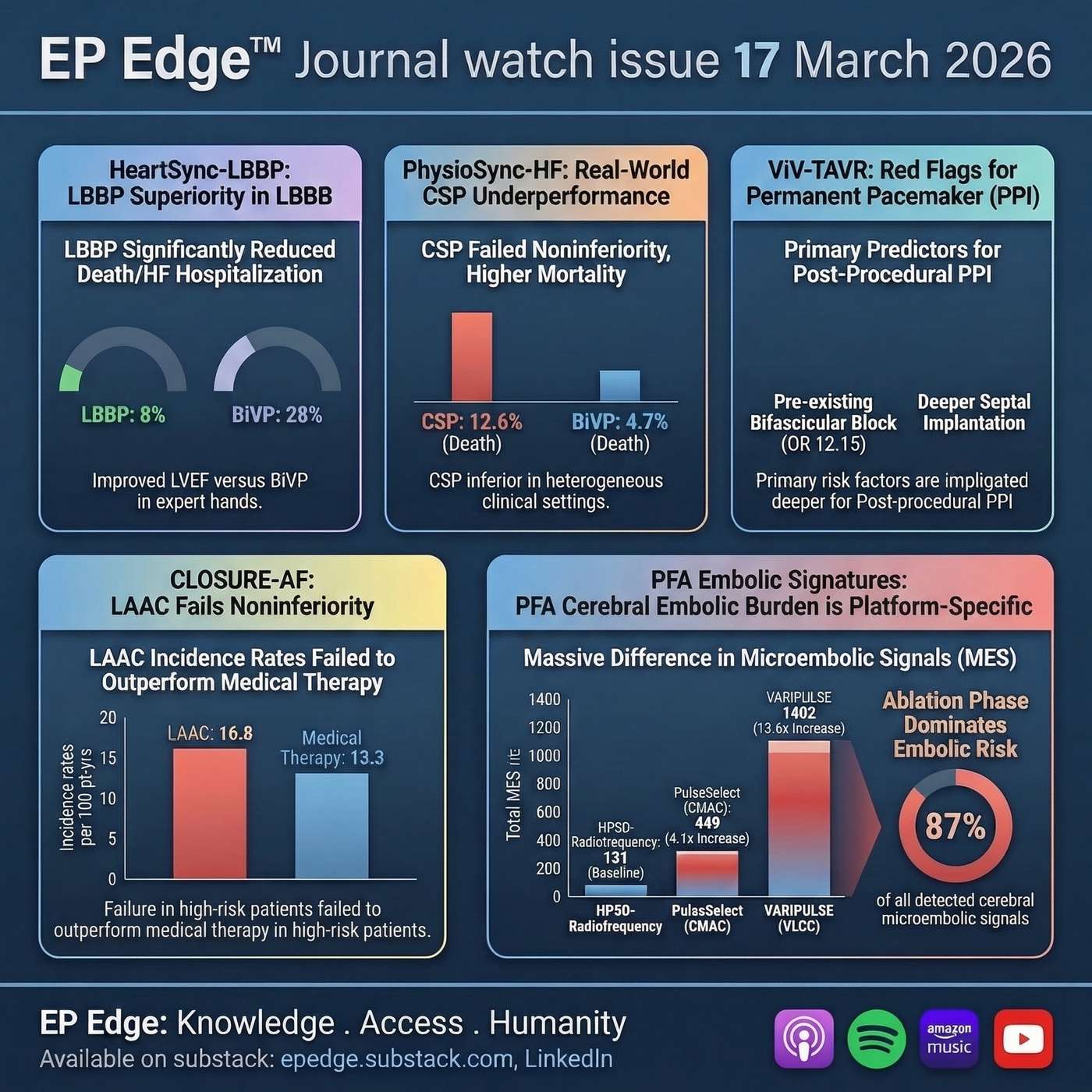 EP Edge Journal Watch Issue 17 April 2026: CLOSURE-AF, Left Atrial Appendage Closure vs Medical Therapy, CRT Pacing Trials, PFA Cerebral Emboli, and ViV-TAVR Pacemaker Risk | In this episode of EP Edge Journal Watch, Dr. Niraj Sharma reviews five clinically important studies spanning atrial fibrillation, structural heart intervention, heart failure pacing, and contemporary ablation safety. The episode opens with CLOSURE-AF, the randomized trial comparing left atrial appendage closure (LAAC) with physician-directed best medical therapy in older, high-risk patients with atrial fibrillation. The discussion examines whether LAAC can truly match or surpass modern anticoagulation-based care for stroke prevention, why the anticipated bleeding advantage did not clearly materialize, and how these findings should recalibrate clinical thinking around left atrial appendage closure and Watchman-era device strategies in 2026.The episode then turns to cardiac resynchronization therapy and the ongoing debate over conduction system pacing versus conventional biventricular pacing. Dr. Sharma contrasts the HeartSync-LBBP randomized trial with PhysioSync-HF, two studies that move in opposite directions and together provide a practical reality check for electrophysiologists. Key themes include left bundle branch pacing, conduction system pacing, operator experience, reverse remodeling, heart-failure hospitalization, and whether left bundle branch area pacing is ready to replace biventricular pacing as the default CRT strategy.The final segments focus on procedural safety and conduction risk. A mechanistic study comparing pulsed field ablation with high-power short-duration radiofrequency ablation evaluates cerebral micro-embolization detected by transcranial Doppler, emphasizing that embolic burden may be platform-specific rather than a generic property of PFA. The episode also reviews predictors of permanent pacemaker implantation after valve-in-valve TAVR, including bifascicular block, deeper septal implantation, and new bundle-branch block after the procedure. This episode is especially relevant for clinicians interested in atrial fibrillation, LAAC, CRT, conduction system pacing, pulsed field ablation, cerebral embolic risk, and TAVR-related conduction disease. | 23m 09s | ||||||
| 3/30/26 | 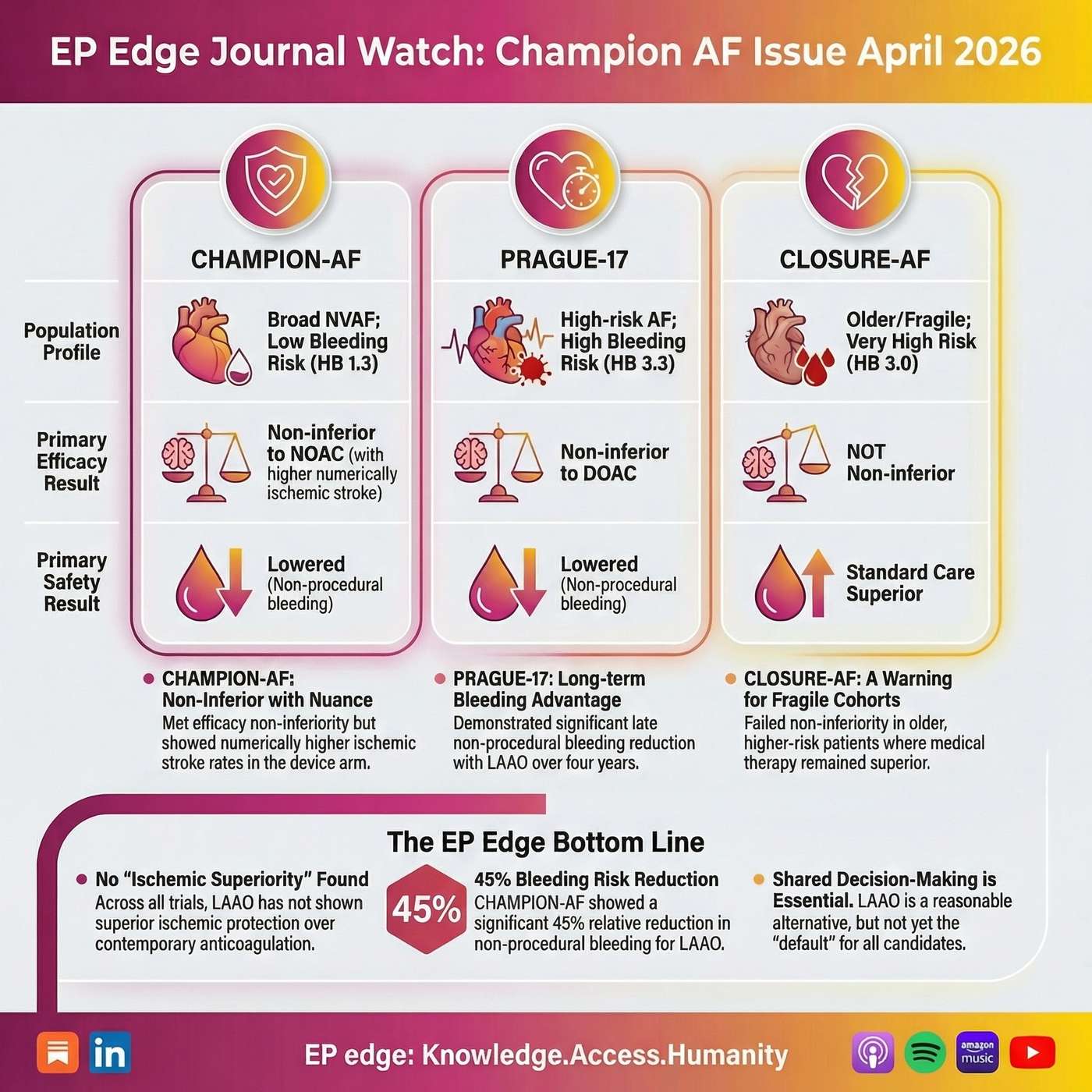 EP Edge™ Journal Watch Breaking News Special Edition: CHAMPION-AF, PRAGUE-17, and CLOSURE-AF — LAAC vs DOACs in Atrial Fibrillation | In this EP Edge™ Journal Watch Breaking News Special Edition, Dr. Niraj Sharma delivers an in-depth analysis of the CHAMPION-AF trial and places its findings in direct comparative context with PRAGUE-17 and CLOSURE-AF, three pivotal randomized studies shaping the modern debate around left atrial appendage closure (LAAC/LAAO) versus direct oral anticoagulants (DOACs) for stroke prevention in atrial fibrillation.This episode goes well beyond a simple trial summary. It examines whether percutaneous left atrial appendage closure can truly challenge contemporary DOAC-first management in patients with nonvalvular atrial fibrillation, and whether the latest evidence justifies broader expansion of LAAC in routine electrophysiology practice. The discussion focuses on the real clinical questions facing electrophysiologists, cardiologists, and stroke prevention specialists in 2026: Which patients remain best served by oral anticoagulation? Where does LAAC still have a meaningful role? And how should clinicians interpret noninferiority claims when ischemic events, bleeding definitions, and procedural risk tell a more complicated story?The episode begins with a detailed breakdown of CHAMPION-AF, including trial design, patient selection, baseline stroke and bleeding risk, endpoint construction, and the interpretation of the primary efficacy and safety results. Particular attention is given to the noninferiority framework, the absolute margin used in the study, the numerical ischemic stroke signal in the device arm, the distinction between procedure-related and non–procedure-related bleeding, and the critical question of whether the reported bleeding advantage is robust enough to offset the upfront risk of device implantation. The discussion also explores why the lack of drug-specific DOAC breakdown matters when interpreting a comparator arm labeled broadly as “NOAC therapy.”The episode then turns to PRAGUE-17, a landmark randomized comparison of LAAC versus DOAC therapy in high-risk atrial fibrillation patients, and explains why it remains one of the strongest supportive trials for selective LAAC use. Dr. Sharma reviews the long-term follow-up, the late divergence in nonprocedural bleeding, the importance of the apixaban-dominant comparator arm, and why PRAGUE-17 supports careful patient selection rather than routine substitution of LAAC for anticoagulation.The analysis then addresses CLOSURE-AF, a major counterweight in this space and arguably one of the most clinically relevant studies for real-world decision-making. In an older, frailer, higher-risk atrial fibrillation cohort, CLOSURE-AF did not establish a compelling advantage for LAAC over medical therapy. This episode explains why that matters, how procedural risk and early harm affect interpretation, and why CLOSURE-AF materially raises the evidentiary bar for any effort to expand LAAC indications.Across all three trials, this EP Edge™ Journal Watch special edition provides a true comparative analysis of CHAMPION-AF, PRAGUE-17, and CLOSURE-AF, highlighting differences in population risk, device strategy, endpoint design, bleeding definitions, ischemic outcomes, and external validity. The goal is not simply to ask whether LAAC “works,” but to determine where LAAC fits in the actual clinical flow of contemporary atrial fibrillation care.This episode is ideal for listeners seeking a high-level, clinically grounded discussion of atrial fibrillation stroke prevention, Watchman FLX, left atrial appendage occlusion, LAAC versus DOACs, noninferiority trial interpretation, bleeding risk, ischemic stroke outcomes, and evidence-based patient selection in electrophysiology practice.For electrophysiologists, cardiologists, fellows, APPs, and clinicians following the evolving literature on CHAMPION-AF, PRAGUE-17, and CLOSURE-AF, this special edition offers a nuanced, data-driven perspective on one of the most important current controversies in heart rhythm medicine. | 27m 13s | ||||||
| 3/23/26 | 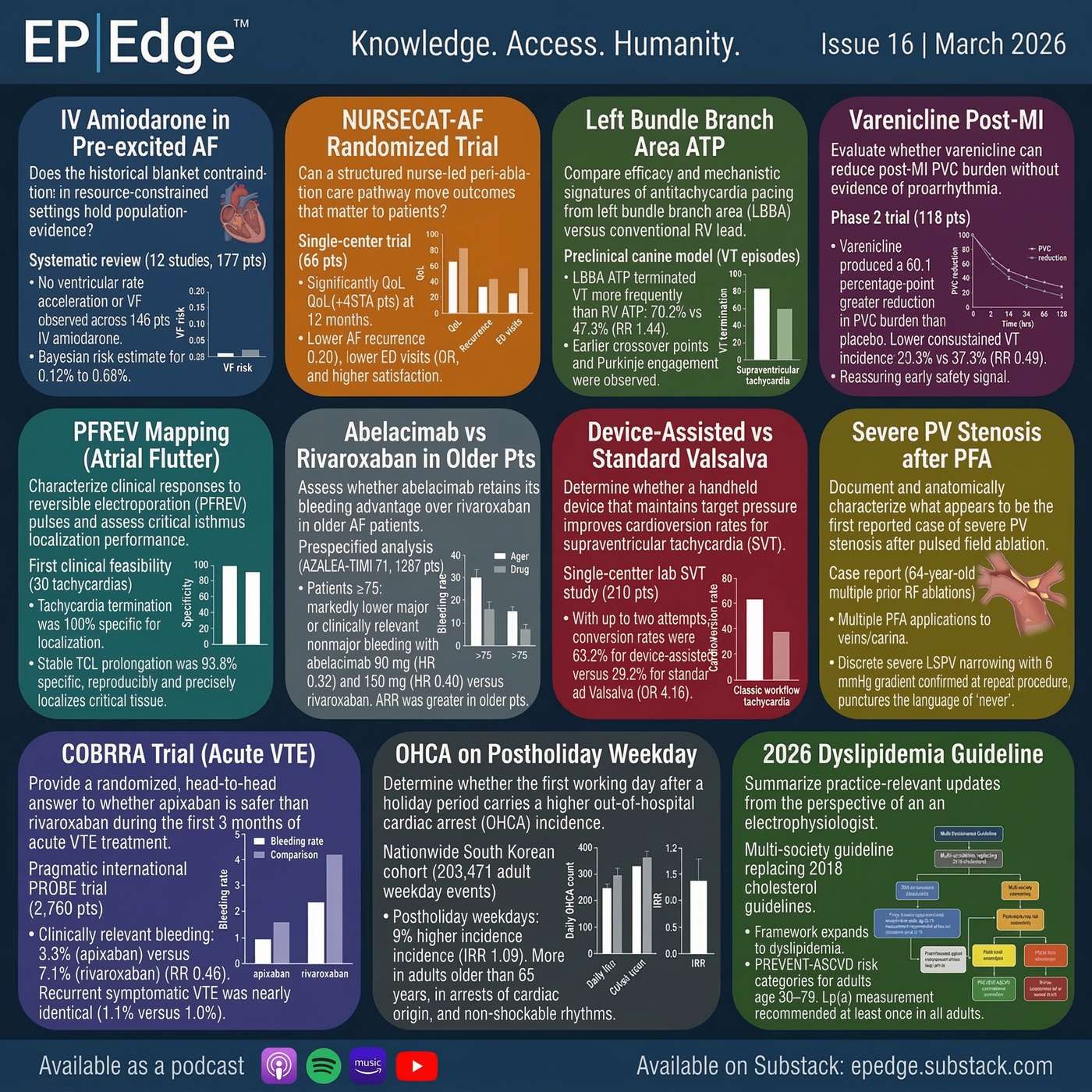 EP Edge Journal Watch Issue 16: 11 New EP Trials on AF Ablation, SVT, Anticoagulation, PFA Safety, VT Pacing, and OHCA | In this episode of EP Edge Journal Watch, Dr. Sharma reviews 11 important new studies shaping modern cardiac electrophysiology, arrhythmia care, and cardiovascular risk management. This March 2026 issue covers intravenous amiodarone in preexcited atrial fibrillation, the NURSECAT-AF randomized trial of nurse-led care after AF ablation, left bundle branch area antitachycardia pacing vs right ventricular ATP, varenicline for ventricular ectopy after myocardial infarction, and the first clinical experience with reversible electroporation mapping in atrial flutter.The episode also examines abelacimab vs rivaroxaban in older patients with atrial fibrillation from AZALEA-TIMI 71, device-assisted vs standard Valsalva for supraventricular tachycardia, the first reported case of severe pulmonary vein stenosis after pulsed field ablation, and the COBRRA trial comparing apixaban vs rivaroxaban bleeding risk in acute venous thromboembolism. Rounding out the issue are a nationwide analysis of out-of-hospital cardiac arrest on the first weekday after holidays and why the 2026 ACC/AHA multisociety dyslipidemia guideline matters directly to EP clinicians.This is a practical, evidence-focused review of where electrophysiology is heading: smarter AF care pathways, safer anticoagulation, better mapping, more physiologic pacing, improved SVT management, and a broader understanding of sudden cardiac risk.Full newsletter: EP Edge Journal Watch with references and infographics is available on LinkedIn as well as on Substack, epedge.substack.com.If you want, I can also make this into a shorter Transistor version, a more keyword-dense SEO version, or a more polished Apple/Spotify-style episode summary. | 22m 06s | ||||||
| 3/16/26 | 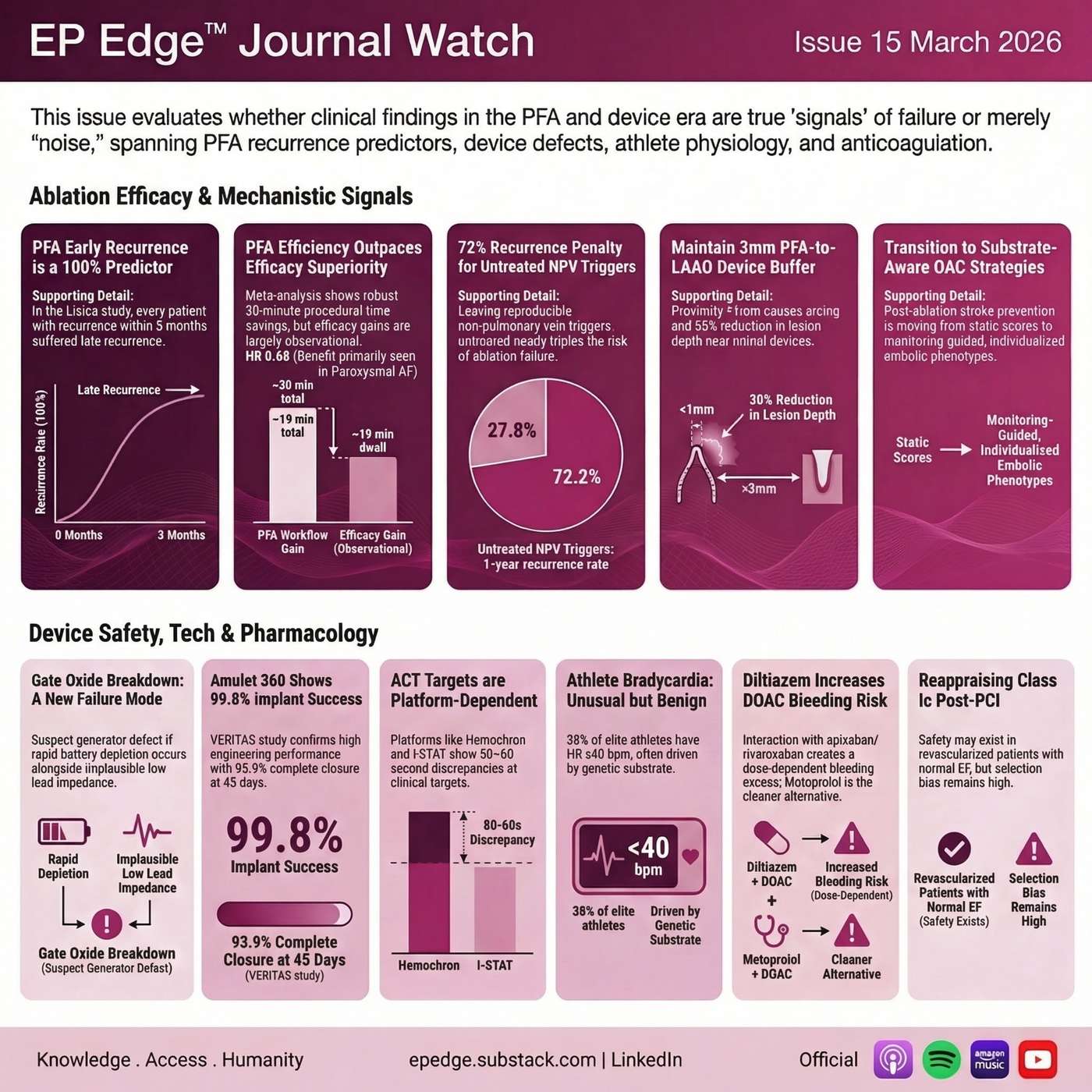 EP Edge™ Journal Watch Issue 15: PFA Recurrence, Bayesian AF Ablation, Non-PV Triggers, Diltiazem-DOAC Risk, and Stroke Prevention After AF Ablation | In EP Edge™ Journal Watch Issue 15, Dr. Niraj Sharma reviews some of the most important new studies in electrophysiology and atrial fibrillation management from March 2026. This episode explores whether early recurrence after pulsed field ablation (PFA) should still be viewed as part of a traditional blanking period or whether it may represent an early marker of later treatment failure. It also examines a Bayesian meta-analysis comparing PFA with thermal ablation, with practical discussion on what Bayesian statistics actually mean for clinicians and how probability-based interpretation may differ from standard p-value thinking.The episode also takes a closer look at the significance of non-pulmonary vein triggers in first-time AF ablation, especially the clinical consequences of identifying reproducible triggers that are not ultimately ablated. Additional featured studies include a provocative reassessment of Class Ic antiarrhythmic therapy after PCI, a clinically important report on rapid battery depletion and CIED generator-related defects, and early performance data on the next-generation Amulet 360 left atrial appendage occlusion device.Other key topics include the procedural implications of performing PFA near metallic LAAO devices, why activated clotting time (ACT) values may not be interchangeable across different testing platforms, and what new data tell us about athlete bradycardia, including the possible interplay between endurance training, physiologic remodeling, and genetic predisposition. The episode also reviews the growing evidence that diltiazem combined with factor Xa inhibitors such as apixaban or rivaroxaban may increase bleeding risk, an issue with direct day-to-day prescribing relevance.Finally, this issue closes with a broader synthesis of OCEAN, ALONE AF, and OPTION, exploring what these studies may mean for the future of stroke prevention after AF ablation and whether post-ablation anticoagulation decisions are moving toward a more individualized model based on rhythm status, stroke risk, bleeding liability, and left atrial appendage management.This is a high-yield podcast for electrophysiologists, cardiologists, fellows, advanced practice providers, and clinicians interested in AF ablation, pulsed field ablation, LAAO, anticoagulation, cardiac devices, and evidence-based heart rhythm management. | 20m 21s | ||||||
| 3/9/26 | 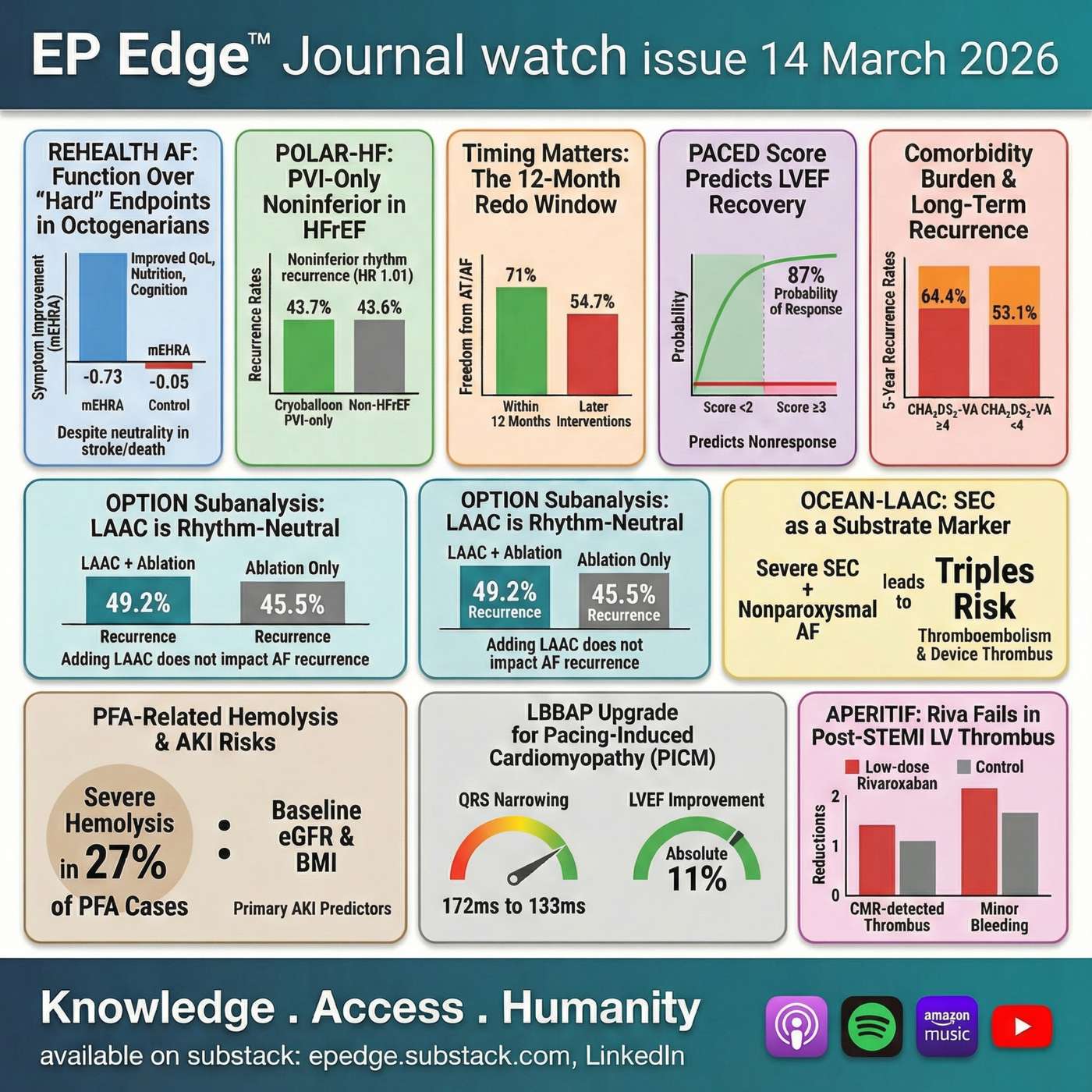 EP Edge Journal Watch #14 (March 2026): AF Ablation at the Extremes: Octogenarians, HFrEF PVI-Only, LAAC, PFA Hemolysis/AKI & Redo Timing | In EP Edge Journal Watch Issue 14 (March 2026), Dr. Niraj Sharma breaks down the most clinically “edge-case” decisions in contemporary electrophysiology—where ablation strategy, stroke prevention, and safety monitoring collide.This episode covers:AF ablation in octogenarians (REHEALTH AF): why the signal may be less about short-term hard outcomes and more about symptoms, function, and patient-centered endpoints.Heart failure + AF (POLAR-HF): the case for a standardized PVI-only approach in HFrEF—and when simplicity is the point.LAAC after ablation (OPTION subanalysis): whether left atrial appendage closure changes AF recurrence (and why rhythm success ≠ stroke immunity).Severe spontaneous echo contrast before LAAC (OCEAN-LAAC): when “smoke” is a high-risk biology phenotype that should change surveillance and post-device antithrombotic strategy.Multimorbidity and PVI: what long-term recurrence really looks like in high comorbidity-burden patients—and how to reset goals toward AF burden and symptoms.Pulsed field ablation safety: hemolysis markers (haptoglobin depletion), AKI risk under routine hydration, and who needs tighter post-procedure monitoring (Farapulse vs PulseSelect).Redo ablation timing: evidence that earlier repeat ablation after recurrence may improve rhythm and quality-of-life outcomes.Plus: PACED score for LVEF recovery after AF ablation, LBBAP upgrades for pacing-induced cardiomyopathy, and a cardiology bonus trial (APERITIF) on LV thrombus prevention after anterior STEMI.References and visuals are available with the newsletter on LinkedIn and on Substack (epedge.substack.com). | 33m 26s | ||||||
| 3/2/26 | 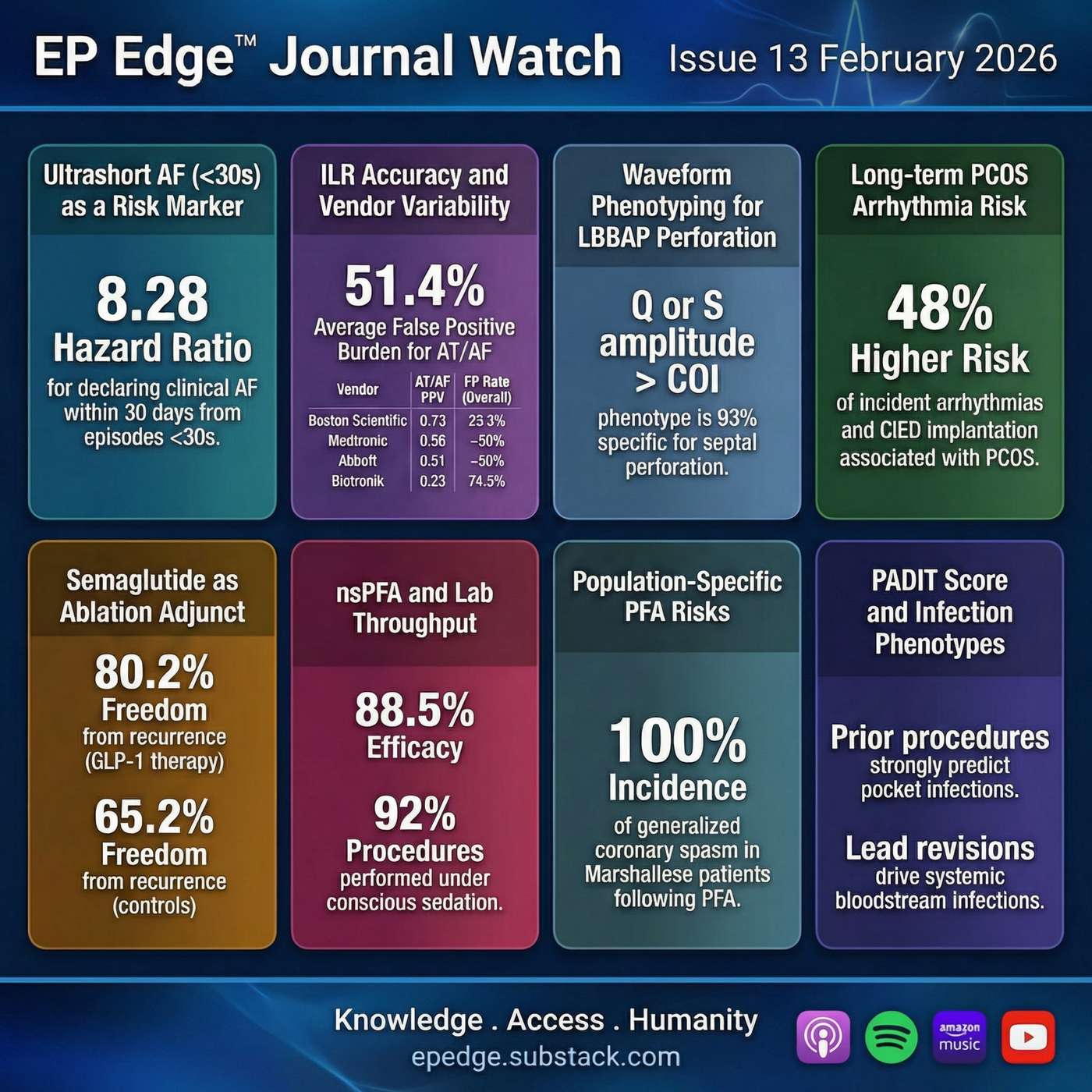 EP Edge Journal Watch Issue 13 (March 2026): Ultrashort AF, ILR Accuracy, Semaglutide + Ablation, PADIT, PCOS, LBBAP and Next-Gen nanosecond PFA (SCENA-AF) | EP Edge Journal Watch — Issue 13 (March 2026) explores a core 2026 EP problem: signal detection (wearables, patches, ILRs) and energy delivery (next-gen PFA) are advancing faster than the clinical rules we use to interpret risk and outcomes. In this episode, Dr. Niraj Sharma breaks down what’s clinically actionable, what’s methodologically fragile, and what should change practice now versus what needs better evidence.Topics covered (high-level):Ultrashort atrial arrhythmias (<30 seconds) and what they may imply on continuous monitoringImplantable loop recorder (ILR) “AF alerts” and why vendor performance is not interchangeable Semaglutide (GLP-1) and AF ablation in obesity: metabolic modulation as an EP strategy, not an afterthoughtNanosecond pulsed field ablation (nsPFA) for paroxysmal AF (SCENA-AF) and what it means for workflow (including anesthesia strategy) A high-stakes coronary spasm signal in a population-enriched cohortLBBAP perforation detection: interpreting iEGMs as phenotype, not just amplitude PADIT score validation by infection subtype—toward phenotype-aware preventionPCOS and long-term arrhythmia risk: a women’s cardiovascular EP domain hiding in plain sight Read the full newsletter (graphics + references): epedge.substack.com Subscribe on LinkedIn (EP Edge Journal Watch): https://lnkd.in/e-Wa4diC Subscribe to EP Edge (Monthly Deep Dives): https://lnkd.in/ep3NdZUzSubscribe Substack: epedge.substack.com | 23m 30s | ||||||
| 2/23/26 | 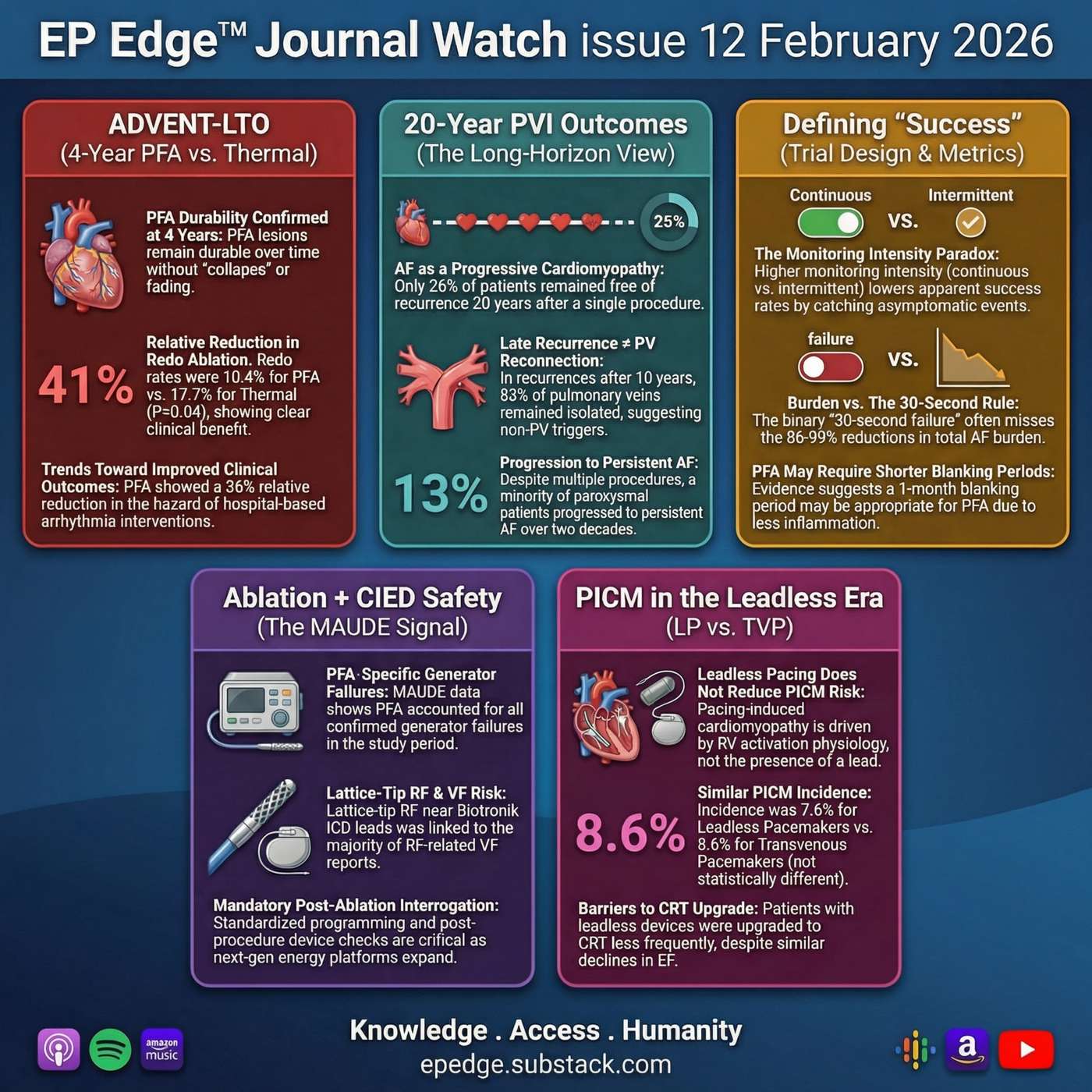 EP Edge™ Journal Watch: February 2026 Issue 12: AF Ablation “Success” Reframed: ADVENT-LTO 4-Year PFA Durability, 20-Year PVI Outcomes, Monitoring Rules, CIED Risks & PICM | In this episode of EP Edge™ Journal Watch (Issue 12, February 2026), Dr. Niraj Sharma breaks down a deceptively simple question in atrial fibrillation (AF) ablation: what does “success” actually mean—at 1 year, 4 years, and 20 years? We start with ADVENT-LTO, the long-term extension of the randomized ADVENT trial, examining 4-year outcomes of pulse field ablation (PFA) vs thermal ablation—and why redo ablation and hospital-based interventions may matter more than a single headline p-value.Next, we zoom way out with a 20-year pulmonary vein isolation (PVI) cohort, showing how AF behaves like a progressive atrial cardiomyopathy over decades—and why very late recurrences may occur even when PV isolation remains durable.Then we tackle the “quiet drivers” of trial results: monitoring intensity, the 30-second recurrence rule, blanking periods, and AF burden—the design choices that can make technologies look better (or worse) without changing biology.Finally, two practical, real-world segments: ablation in patients with pacemakers/ICDs (MAUDE signal patterns, including resets and generator issues) and pacing-induced cardiomyopathy (PICM) in the leadless era (leadless vs transvenous RV pacing). Full written issue (with references) is on Substack: epedge.substack.com and on LinkedIn Newsletter EP Edge Journal Watch | 24m 48s | ||||||
| 2/19/26 | 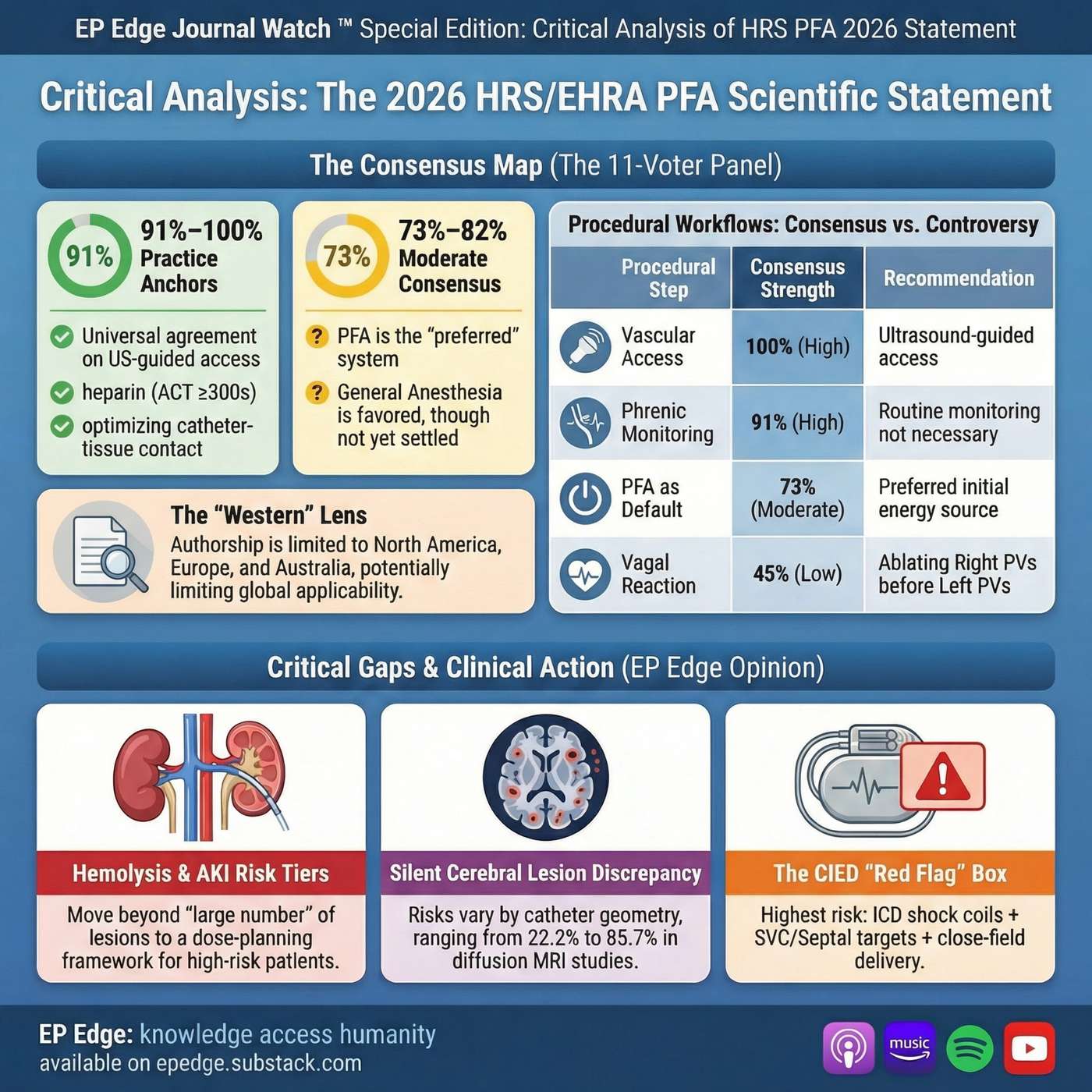 EP Edge™ Journal Watch (Special Edition): Feb 2026 HRS/EHRA Pulsed Field Ablation (PFA) Scientific Statement — Vote Counts, Safety Signals, and Real-World Workflow | In this EP Edge™ Journal Watch Special Edition, we unpack the newly released 2026 HRS/EHRA Scientific Statement on Pulsed Field Ablation (PFA) and translate “consensus language” into practical, lab-ready decision-making. This isn’t a surface summary—it’s a critical appraisal of how the statement was built (including the 11-voter model), where the field is truly aligned, and where recommendations may outpace either the evidence base or global clinical reality. final pfa statementYou’ll hear a Consensus Map that separates high-agreement anchors (e.g., access, anticoagulation, sheath discipline) from moderate-consensus workflow preferences (e.g., anesthesia models, ICE use, waiting periods), and the genuinely controversial areas. Then we go deep on what matters most to operators and patients: platform-aware safety and post-market signal management, hemolysis/AKI mitigation tied to lesion burden, phrenic/airway realities, esophageal considerations when lesion sets expand, CIED interaction risk, and why “PFA is a system, not a single technology” should change how you read every recommendation. final pfa statementShow notes: All graphics and full references are available on epedge.substack.com and on LinkedIn in the EP Edge™ Journal Watch newsletter (Issue 12 Special Edition). Questions/suggestions: email: epedgecast@gmail.com | 16m 41s | ||||||
| 2/16/26 | 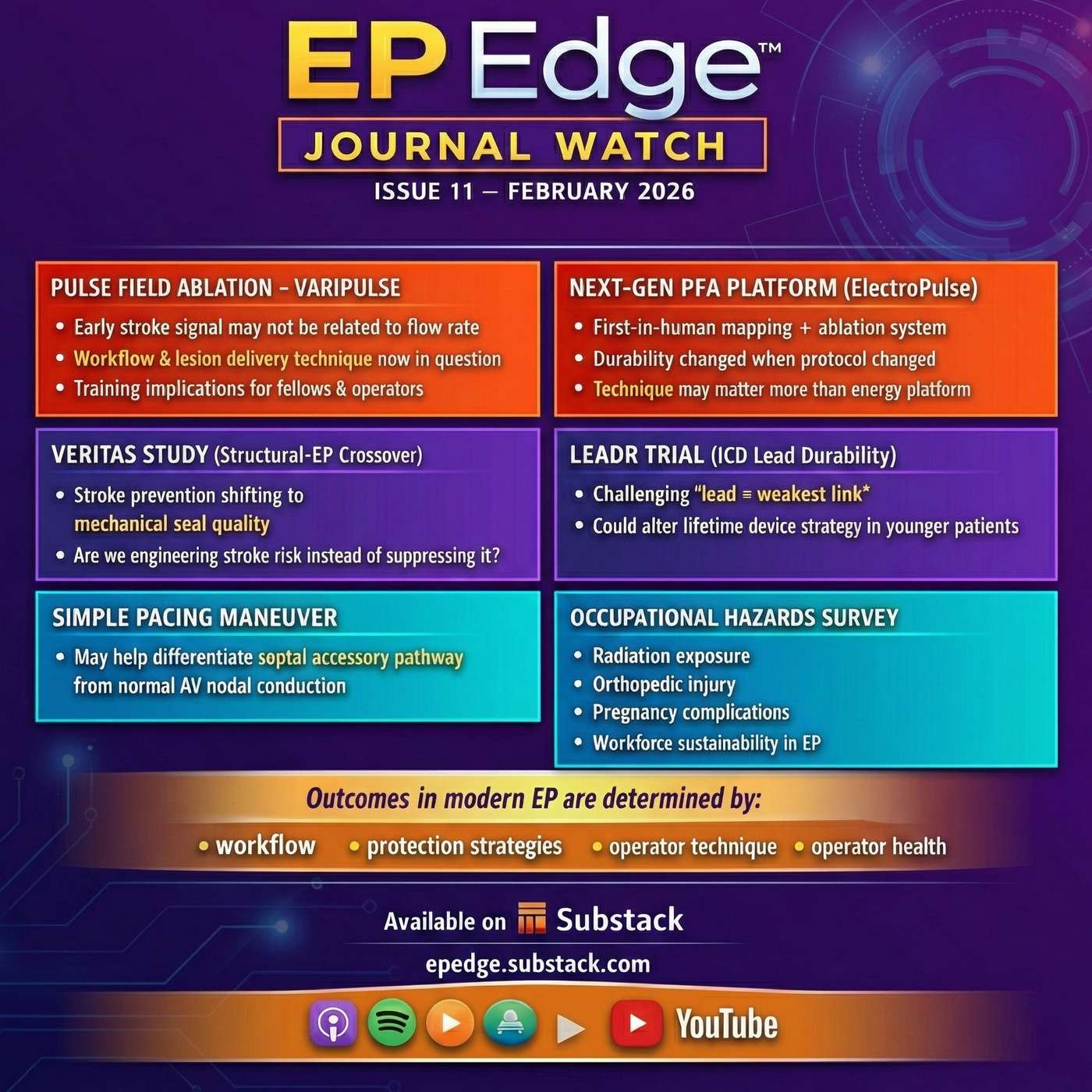 EP Edge Journal Watch Issue 11 February 2026: Varipulse Safety Signal, ElectroPulse PFA, Farapoint CTI Ablation, Leadless Pacemaker Infection & EP Occupational Hazards | In this episode of EP Edge Journal Watch, we review several developments that directly impact modern electrophysiology practice — from pulsed field ablation safety to operator health. We begin with the real-world Varipulse experience, where early neurovascular events dropped dramatically after workflow modification and reduction of lesion stacking, highlighting that PFA success depends as much on procedural execution as on device design. We then discuss the first-in-human ElectroPulse mapping-ablation platform and what its early durability signals suggest about integrated catheter systems and standardized ablation protocols. We next turn to right-sided ablation safety. The episode examines cavotricuspid isthmus pulsed field ablation, the mechanism of coronary vasospasm, and the high-dose nitroglycerin protection strategy used in studies. We also review emerging intracoronary imaging findings suggesting possible delayed coronary arterial remodeling after PFA. Device and structural therapy updates follow, including Amulet 360 left atrial appendage occlusion sealing performance and long-term outcomes of a small-diameter ICD lead platform designed to improve lead durability. Finally, we discuss practical EP laboratory implications: a simplified pacing maneuver to distinguish AV nodal from septal accessory pathway conduction, the first reported infection involving an atrial leadless pacemaker, and new data on occupational hazards in electrophysiology — including radiation exposure, cataracts, orthopedic injury, and pregnancy-related workforce considerations. The central message is clear: electrophysiology outcomes increasingly depend on workflow discipline, protection strategies, and operator sustainability. Full references, figures, and detailed graphics are available in the LinkedIn Newsletter: EP Edge Journal Watch — Issue 11 (February 2026) and on Substack at epedge.substack.com. Questions or feedback: epedgecast@gmail.com. | 13m 17s | ||||||
| 2/9/26 | 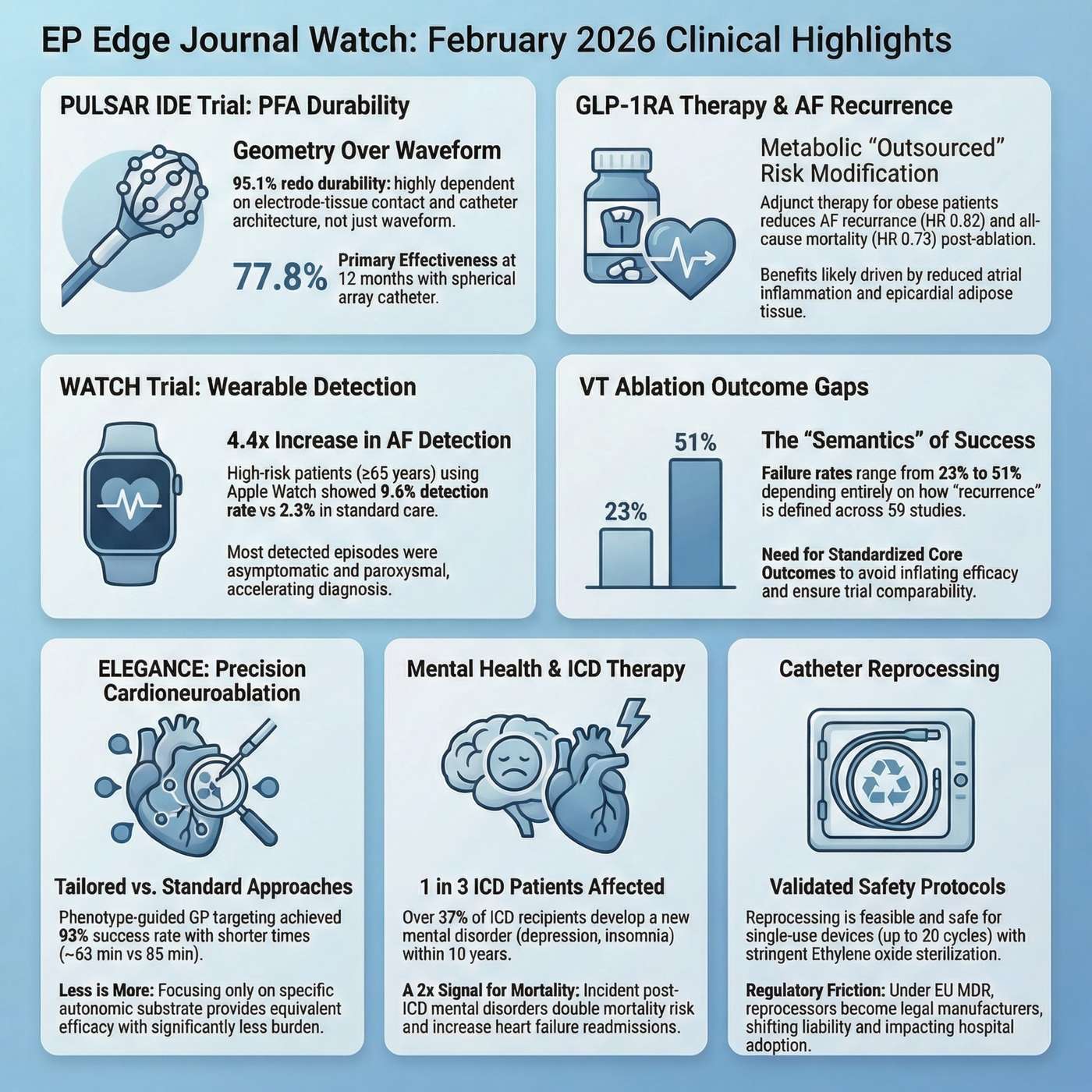 EP Edge Journal Watch Issue 10, February 2026: Pulsed Field Ablation Durability, AF Ablation Outcomes, Wearable AF Detection, ICD and VT Insights | EP Edge Journal Watch: Feb 2026 Issue 10In this episode of EP Edge Journal Watch, we examine the latest developments shaping the future of cardiac electrophysiology, with a focus on pulsed field ablation durability, atrial fibrillation ablation outcomes, wearable AF detection, ventricular tachycardia ablation endpoints, autonomic modulation, and ICD patient outcomes. Pulsed field ablation has rapidly transformed AF ablation due to its safety and efficiency, but long-term success depends on durable pulmonary vein isolation. We explore how next-generation catheter architecture, electrode geometry, and tissue contact optimization are redefining durability and advancing the effectiveness of catheter ablation for atrial fibrillation.This episode also highlights the expanding understanding that atrial fibrillation is driven not only by electrical triggers but also by systemic metabolic and autonomic factors. We discuss how metabolic therapies, including GLP-1 receptor agonists, may improve long-term rhythm control after ablation by modifying atrial substrate and inflammation. In parallel, wearable technologies such as smartwatches are accelerating AF detection, enabling earlier diagnosis of asymptomatic atrial fibrillation and fundamentally changing screening, referral, and management pathways for electrophysiologists and cardiologists.Beyond atrial fibrillation, we explore emerging advances in cardioneuroablation as a precision therapy for functional bradycardia and reflex syncope, the profound clinical impact of mental health disorders on outcomes following ICD implantation, and the ongoing challenges in defining meaningful success metrics in ventricular tachycardia ablation. We also examine the growing importance of sustainability, safety, and regulatory oversight in electrophysiology practice, including the evolving role of catheter reprocessing. Together, these topics reflect a broader transformation in electrophysiology toward an integrated approach that addresses arrhythmia mechanisms, substrate biology, patient physiology, and long-term clinical outcomes.Full references, detailed discussion, graphs, and visual summaries for this episode are available on the EP Edge Journal Watch newsletter on LinkedIn, as well as the full long-form edition now available on Substack at epedge.substack.com. If you have questions, suggestions, or feedback, please email epedgecast@gmail.com. | 25m 46s | ||||||
| 2/6/26 | 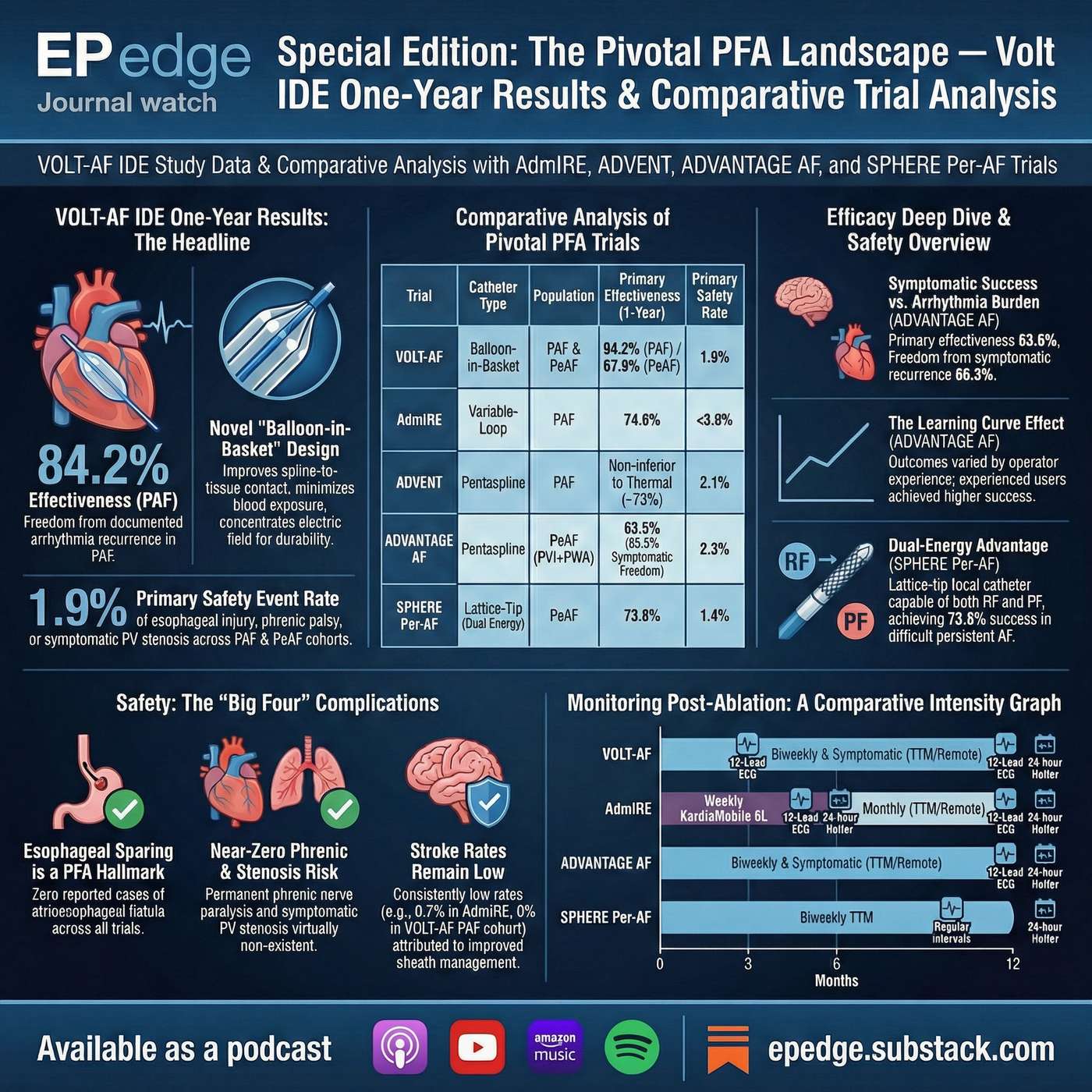 EP Edge Journal Watch Special Edition: VOLT IDE One-Year Results in Context: ADVENT, ADVANTAGE-AF, AdmIRE, SPHERE-Per-AF & U.S. PFA Pivotal Trials | Pulsed field ablation (PFA) has rapidly reshaped atrial fibrillation ablation, but true clinical validation depends on durable one-year outcomes, not early feasibility or acute safety alone. In this EP Edge Journal Watch Special Edition, Dr. Niraj Sharma delivers a comprehensive, system-level analysis of the Abbott VOLT IDE one-year data, now completing the 12-month efficacy and safety landscape across major U.S. PFA platforms.This episode critically reviews and contextualizes results from the VOLT IDE trial alongside other pivotal and near-pivotal studies, including ADVENT, ADVANTAGE-AF, AdmIRE, SPHERE-9 first-in-human, and SPHERE-Per-AF. The discussion spans paroxysmal, persistent, and advanced AF populations, with attention to how ablation strategy (PVI-only vs adjunctive lesions), patient risk profile, and post-ablation monitoring intensity influence reported outcomes.Key themes include one-year efficacy versus composite effectiveness, freedom from atrial arrhythmias, repeat procedures, and major safety endpoints such as stroke, tamponade, and esophageal injury. Rather than ranking technologies, this episode emphasizes methodology, trial design, and clinical context, explaining why efficacy signals differ across studies and how these data should be interpreted in everyday electrophysiology practice.For additional references, detailed tables, graphics, and deeper comparative analysis, visit the LinkedIn EP Edge newsletter and Substack at ephedge.substack.com. If you have suggestions or concerns, you can reach Dr. Sharma at ephedgecast@gmail.com | 9m 26s | ||||||
| 2/2/26 | 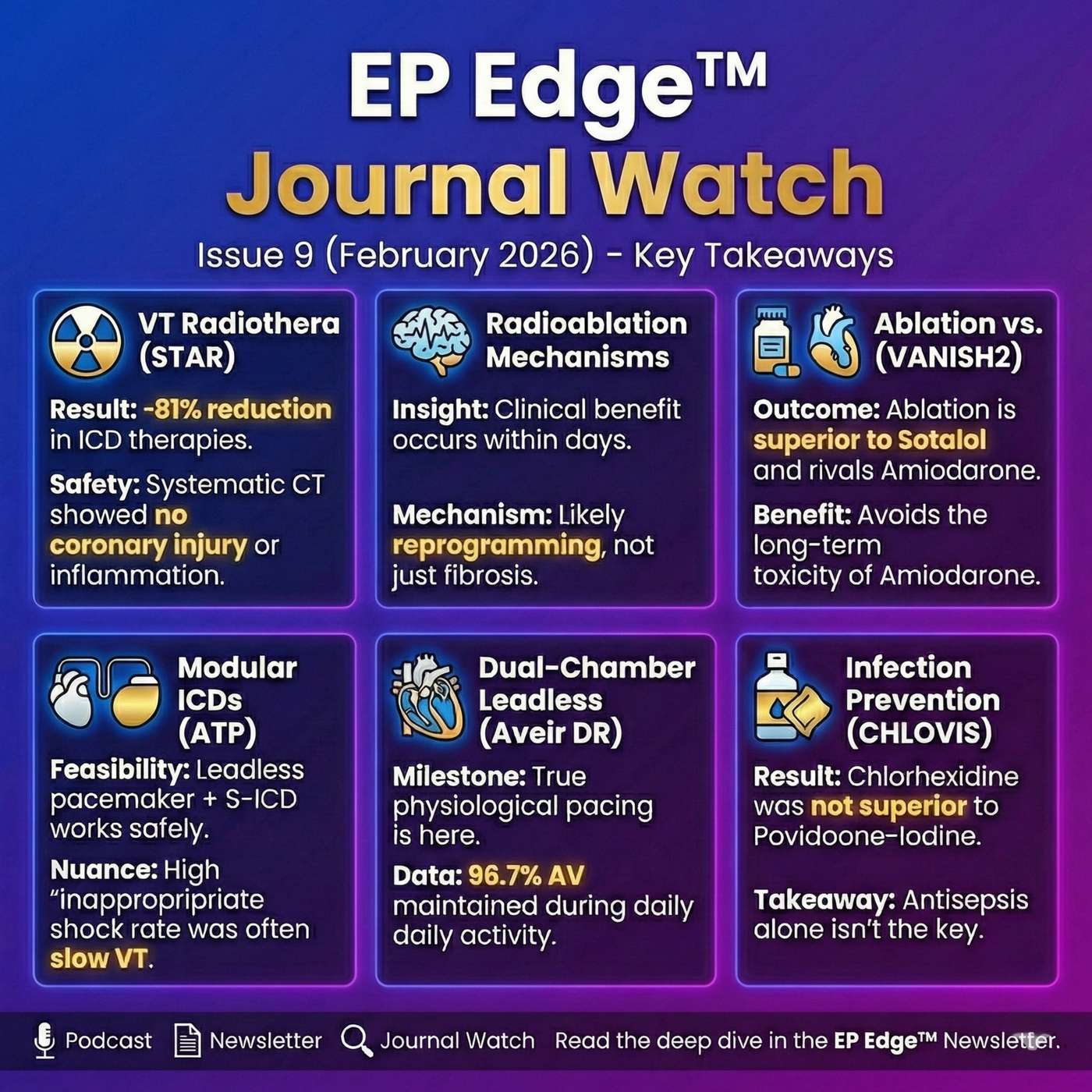 EP Edge Journal Watch — Issue 9 Redefining Ventricular Tachycardia Care: From Noninvasive Radioablation to Leadless, Modular, and Drug-Based Strategies | In EP Edge Journal Watch – Issue 9 (February 2026), we take a comprehensive, clinically grounded look at the evolving management of ventricular tachycardia (VT)—from last-line noninvasive therapies to next-generation devices, pharmacologic strategy, and infection prevention.This episode critically reviews the STRA-MI-VT trial, examining stereotactic arrhythmia radioablation (STAR) for refractory VT with a unique focus on coronary safety using serial coronary CT angiography. We explore why early VT suppression occurs after radioablation and what emerging mechanistic data suggest about electrophysiologic remodeling beyond fibrosis.We then turn to contemporary VT decision-making with a deep dive into the VANISH2 substudy, comparing first-line catheter ablation with antiarrhythmic drug therapy, highlighting where ablation clearly outperforms sotalol and rivals amiodarone—without long-term extracardiac toxicity.Next, we examine modular defibrillation systems combining subcutaneous ICDs with leadless antitachycardia pacing, unpacking ATP effectiveness, complication rates, and the critical nuance behind so-called “inappropriate” therapies. We also review the latest data on dual-chamber leadless pacing, demonstrating high real-world AV synchrony and outlining what questions remain unanswered.The episode concludes with two essential but often under-discussed domains:Why antiarrhythmic drugs still matter in 2026, using updated EHRA frameworks for safer, more rational useWhat the CHLOVIS trial teaches us about CIED infection prevention—and why skin antisepsis alone is not the decisive factorAs always, EP Edge Journal Watch prioritizes clinical context, trial design, limitations, and practical implications, helping electrophysiologists cut through signal versus noise. Looking for More Detail?For expanded references, trial tables, figures, and visual summaries, visit the EP Edge Journal Watch LinkedIn Newsletter. Each study discussed in this episode is accompanied there by:Trial-at-a-glance summariesKey graphs and imaging highlightsStructured critical appraisalClinical interpretation beyond the abstractIf you prefer to read, review figures, or reference the data later, the LinkedIn newsletter is the ideal companion to this podcast episode.If you have questions, feedback, or clinical thoughts, feel free to reach out directly at epedgecast@gmail.com | 12m 46s | ||||||
| 1/26/26 | 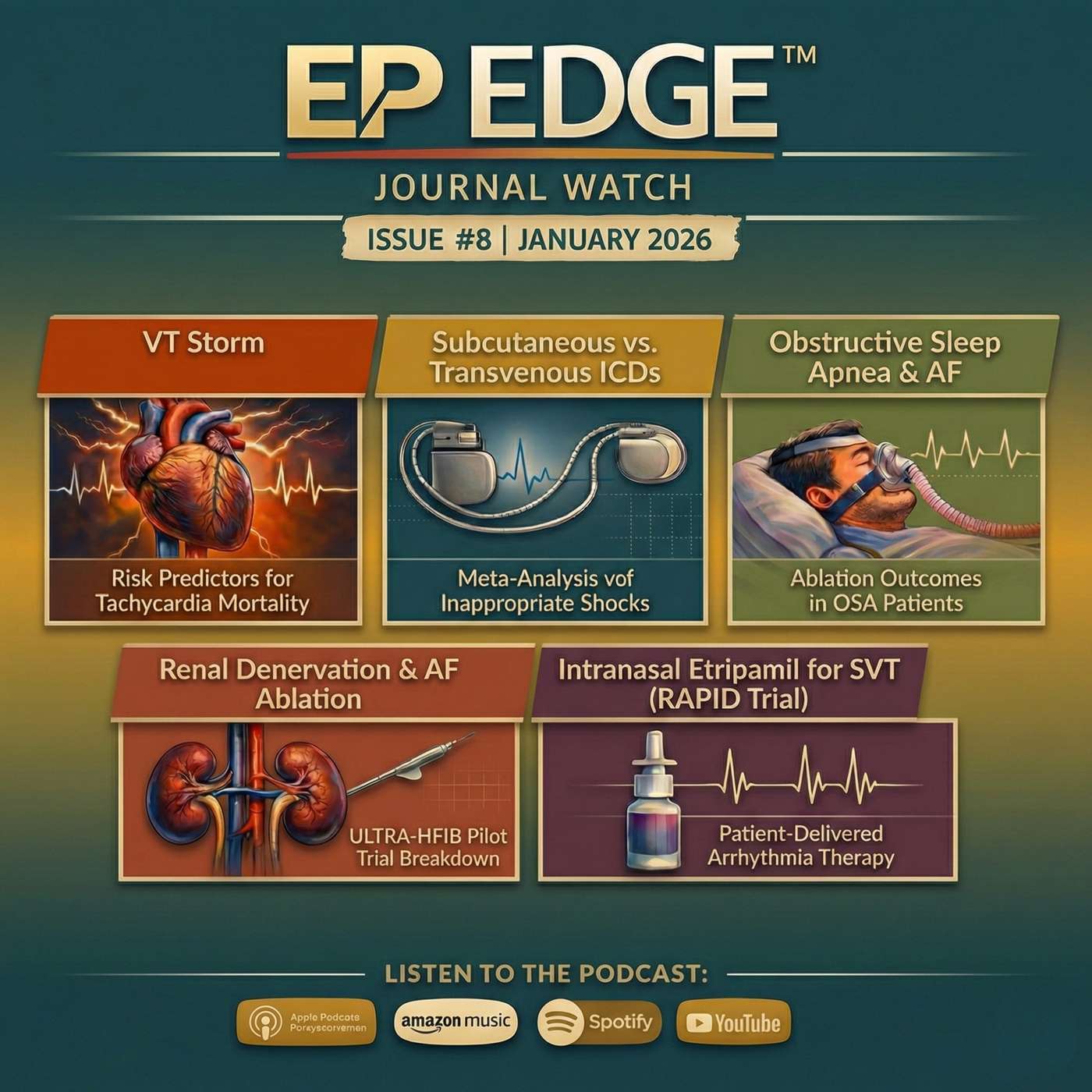 EP Edge Journal Watch – Issue 8 (2026): VT Storm Outcomes, Inappropriate ICD Shocks, AF Ablation Modifiers, and the Rise of Patient-Directed SVT Care | In EP Edge Journal Watch – Issue 8 (2026), we deliver a comprehensive, evidence-driven analysis of the most important and practice-shaping studies in contemporary cardiac electrophysiology.This episode begins with ventricular tachycardia storm, examining why in-hospital mortality remains high despite aggressive rhythm control. We break down the CHAMPS score, focusing on patient selection, systemic illness, statistical modeling, and what the data truly reveal about ablation timing, competing risks, and survival.We then turn to implantable cardioverter-defibrillators, exploring long-term outcomes and real-world trade-offs between subcutaneous and transvenous ICD systems. A detailed discussion of inappropriate shock mechanisms highlights the balance between lead durability, sensing biology, atrial arrhythmias, oversensing, and device programming strategies that matter over years—not months.The episode moves into atrial fibrillation beyond pulmonary vein isolation. We analyze adjunctive renal denervation during AF ablation, reviewing trial methodology, statistical power, and why biologic plausibility does not always translate into clinical significance. We also examine atrial fibrillation outcomes in patients with obstructive sleep apnea, addressing large observational datasets, propensity matching, effect sizes, and the critical distinction between association and causation.Practical electrophysiology extends into the emergency department as well. This episode reviews data on preventing diltiazem-induced hypotension in atrial fibrillation with rapid ventricular response, focusing on physiologic rationale, dosing considerations, and where this strategy fits into real-world care.Finally, we close with a true paradigm shift in arrhythmia management: patient-delivered therapy for paroxysmal supraventricular tachycardia. We explore how intranasal therapy allows selected patients to terminate SVT outside the hospital, what the trial data support, and how this may reshape care pathways, patient autonomy, and healthcare utilization.Throughout the episode, EP Edge Journal Watch emphasizes study design, statistical interpretation, limitations, and clinical applicability, cutting through hype to deliver insights that matter for practicing electrophysiologists, cardiologists, and advanced trainees.This episode is essential listening for anyone interested in ventricular arrhythmias, ICD therapy, atrial fibrillation ablation, device strategy, emergency rhythm management, and the future of patient-centered electrophysiology care. | 17m 31s | ||||||
Showing 25 of 33
Sponsor Intelligence
Sign in to see which brands sponsor this podcast, their ad offers, and promo codes.
Chart Positions
20 placements across 20 markets.
Chart Positions
20 placements across 20 markets.