
Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Most discussed topics
Brands & references
Total monthly reach
Estimated from 39 chart positions in 39 markets.
By chart position
- 🇺🇸US · Life Sciences#26100K to 300K
- 🇬🇧GB · Life Sciences#34100K to 300K
- 🇨🇦CA · Life Sciences#5330K to 100K
- 🇩🇪DE · Life Sciences#8830K to 100K
- 🇦🇺AU · Life Sciences#1075K to 30K
- Per-Episode Audience
Est. listeners per new episode within ~30 days
289K to 923K🎙 ~2x weekly·84 episodes·Last published 2w ago - Monthly Reach
Unique listeners across all episodes (30 days)
579K to 1.8M🇺🇸16%🇬🇧16%🇨🇦5%+36 more - Active Followers
Loyal subscribers who consistently listen
231K to 738K
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
From 13 epsHost
Recent guests
Recent episodes
Helen Pearson: What Constitutes Real Medical Evidence?
Jun 6, 2026
51m 45s
Assessment of the Hantavirus with Prof Donald Milton
May 14, 2026
52m 02s
Joanna Stern: An AI Immersion for 365 Days
May 13, 2026
58m 08s
Roxanne Khamsi: We Are All Genetic Mosaics
Apr 25, 2026
51m 36s
Sebastian Mallaby: The Infinity Machine
Apr 19, 2026
53m 43s
Social Links & Contact
Official channels & resources
Official Website
Login
RSS Feed
Login
| Date | Episode | Topics | Guests | Brands | Places | Keywords | Sponsor | Length | |
|---|---|---|---|---|---|---|---|---|---|
| 6/6/26 |  Helen Pearson: What Constitutes Real Medical Evidence?✨ | medical evidenceevidence-based medicine+4 | Helen Pearson | NatureUniversity College London+3 | McMaster UniversityCovid | evidence-based medicinebiomedical journalism+3 | — | 51m 45s | |
| 5/14/26 |  Assessment of the Hantavirus with Prof Donald Milton✨ | Hantavirusinfectious diseases+3 | Prof Donald Milton | — | — | HantavirusProf Donald Milton+3 | — | 52m 02s | |
| 5/13/26 |  Joanna Stern: An AI Immersion for 365 Days✨ | AIhealth technology+3 | Joanna Stern | Wall Street JournalNew Things+2 | — | AIhealthcare+5 | — | 58m 08s | |
| 4/25/26 |  Roxanne Khamsi: We Are All Genetic Mosaics✨ | genetic mosaicssomatic mutations+3 | Roxanne Khamsi | BEYOND INHERITANCE | — | geneticsmutations+3 | — | 51m 36s | |
| 4/19/26 |  Sebastian Mallaby: The Infinity Machine✨ | AI progressDeepMind+4 | Sebastian Mallaby | AlphaFoldDeepMind+5 | — | AIDeepMind+6 | — | 53m 43s | |
| 4/10/26 |  Trisha Pasricha: How to Get to Poophoria, Making Your Bowel Movements a Joy!✨ | gastroenterologybowel movements+4 | Trisha Pasricha | Harvard Medical SchoolThe Washington Post | — | bowel movementsgut health+6 | — | 56m 49s | |
| 3/29/26 |  On the Future of Species✨ | synthetic biologygenome editing+3 | Adrian Woolfson | GenyroNature Biotechnology+3 | — | synthetic biologygenome sequencing+3 | — | 45m 21s | |
| 3/6/26 |  A Master Class on Sleep✨ | sleep medicinedeep sleep+5 | Yo-El Ju | Washington UniversityHarvard+1 | — | sleepdeep sleep+7 | — | 57m 10s | |
| 2/4/26 |  Robert Wachter & Eric Topol - Discuss a Giant Leap Book✨ | healthmedicine+3 | Robert Wachter | Ground Truths | — | Robert WachterEric Topol+5 | — | 45m 47s | |
| 2/1/26 | 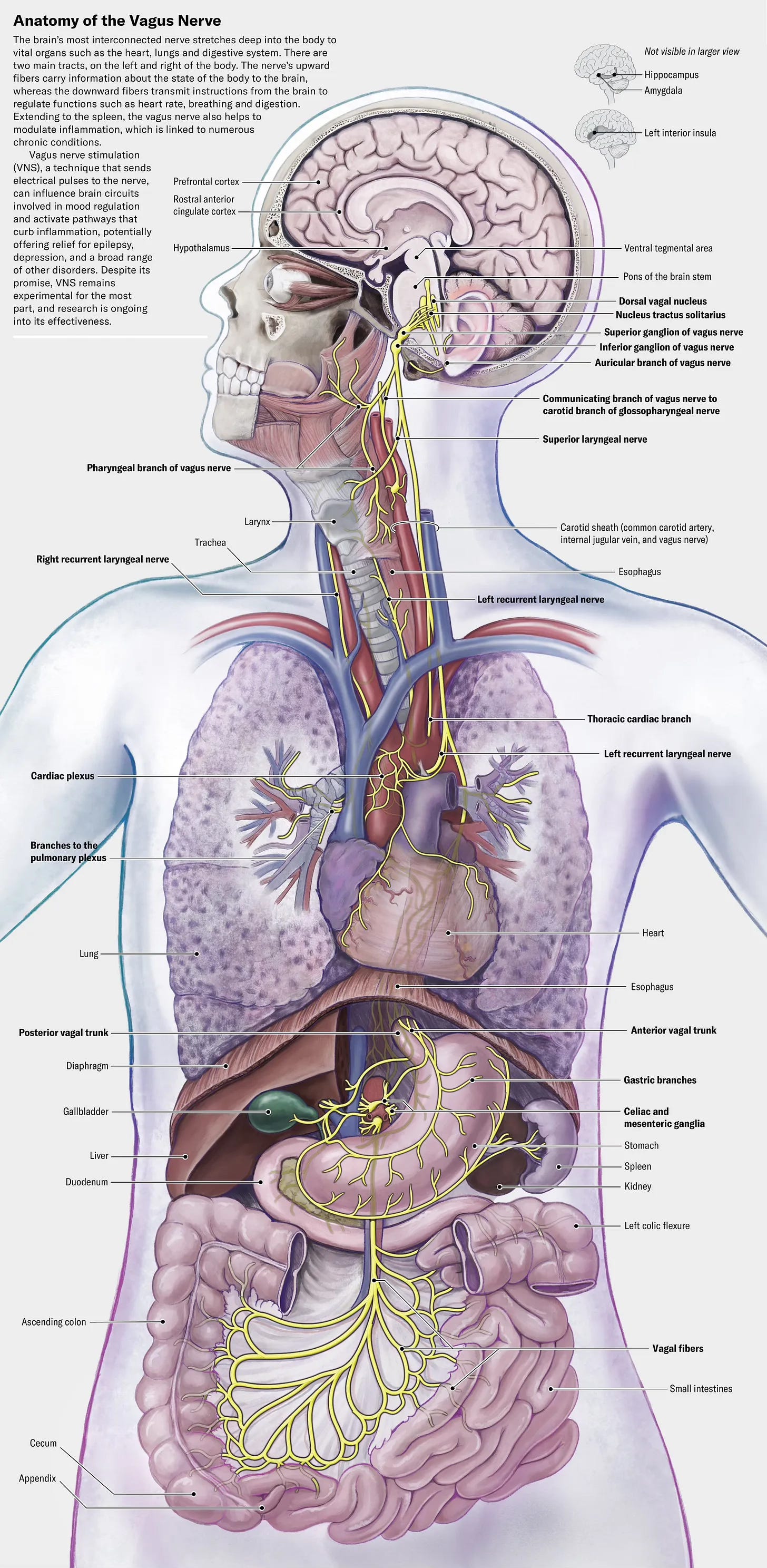 Vagus Nerve Stimulation and the Immune System✨ | vagus nerveimmune system+3 | Dr. Kevin Tracey | Feinstein InstituteNorthwell Health+2 | — | vagus nerveimmune system+3 | — | 1h 03m 59s | |
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 1/18/26 |  A Look Into the Blue Zones✨ | Blue Zoneslongevity+4 | Dan Buettner | Blue Zones LLCAdventist Health+3 | — | Blue Zoneslongevity+5 | — | 55m 31s | |
| 12/21/25 | 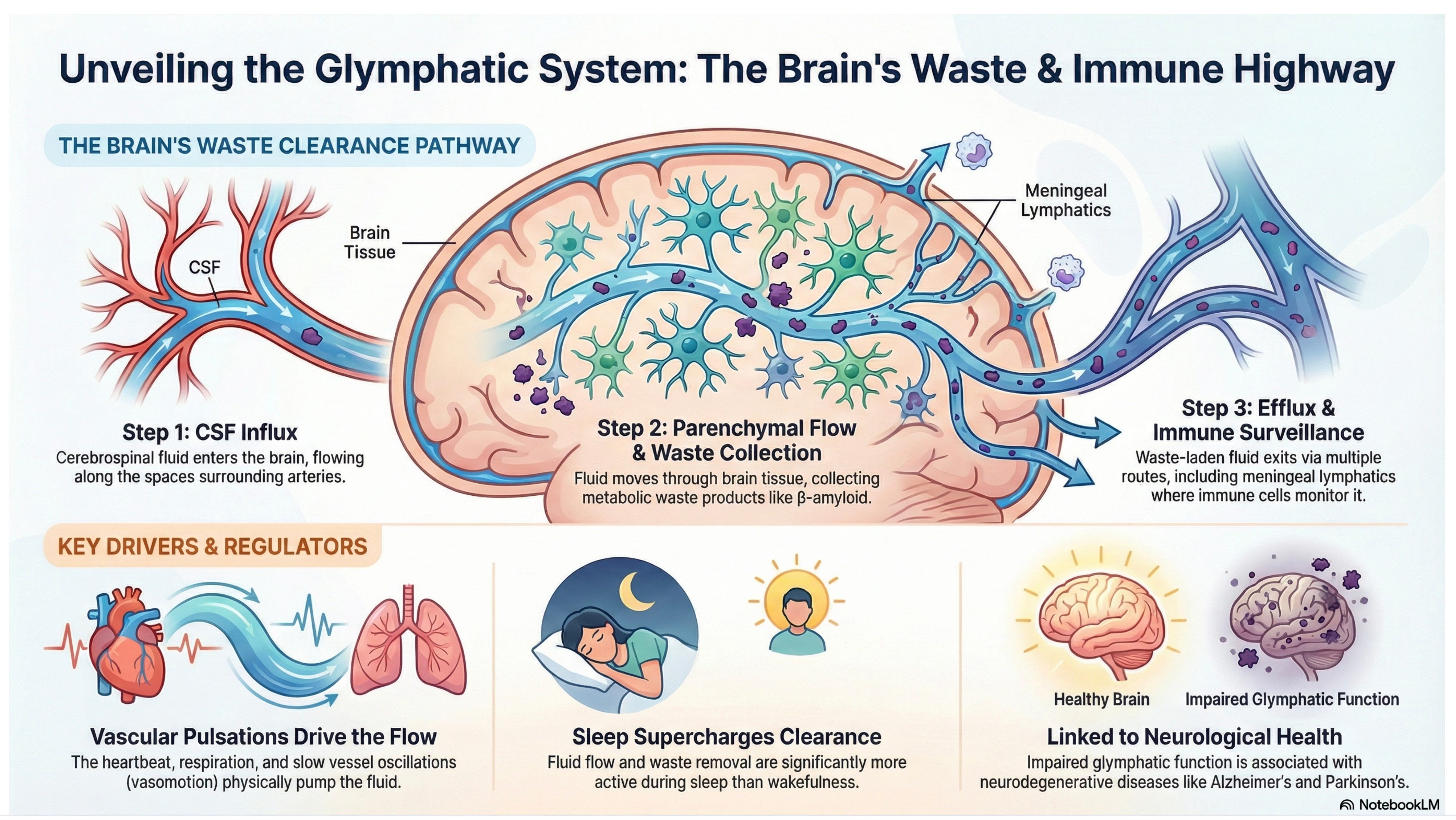 How Our Brain Drains Its Waste Products✨ | brain drainageimmune system+4 | Jonathan Kipnis | Washington UniversityNeuron+3 | — | glymphaticsatrial fibrillation+4 | — | 56m 21s | |
| 12/7/25 |  The Story of Francis Crick, a new masterpiece biography by Matthew Cobb✨ | biographyscience+4 | Matthew Cobb | University of ManchesterThe Astonishing Hypothesis+1 | — | Francis CrickMatthew Cobb+5 | — | 59m 14s | |
| 11/28/25 |  Jennifer Gunter & Eric Topol: Discuss Women’s Health and Recent Changes by FDA for MHT | A couple of weeks ago, the FDA Commissioner published a WSJ oped “The FDA Liberates Women’s Hormone Replacement Therapy” (←gift link) and, with other FDA colleagues, a JAMA essay entitled “Updated Labeling for Menopausal Hormone Therapy” (open-access). That change, and the data cited, led to a series of articles in the days that followed, such as at STAT News “FDA reverses decades-old warning on hormone therapy products for menopause. Agency says the treatments o!fer heart, brain, and bone health benefits” and at the Washington Post “The FDA finally corrects its error on menopause hormone therapy. Women have been needlessly scared away from effective treatments.” If you read through these links, you’ll be confused. Does MHT have proven cognitive benefits? What about a study from 1991 that showed ~50% reduction of fatal heart events with MHT? Or the 35% decreased risk of Alzheimer’s disease? Or the breast cancer increased risk attributed to medroxyprogesterone acetate?I turned to my go-to gynecologist truth teller, Dr. Jen Gunter, to get her review of the evidence. This is a complex topic, with old data from the 2002 Women’s Heath Initiative (WHI), new reports since, population level analysis, changes in preparations of MHT including local delivery, and much more.Here is our conversation which isn’t just about MHT but includes “Big Wellness” marketing direct to middle aged women, the new FDA approved drug for hot flashes, the $14 million cut of the NIH’s Office of Women’s Health , marked increase in philanthropic support of women’s health research, the Surgeon General nominee, ovarian failure, and a lightning round on proven benefits of MHT.Here’s a brief clip on her views of the women’s health “wellness” predatorsWe also discussed the reasons for Dr. Gunter’s planned move next year back to Canada after practicing gynecology for 3 decades in the United States. I referred to a recent GT I wrote about the WHI and the potential favorable impact of MHT on the immune system, as suggested by new data on organ clocks. That finding, which has been replicated, may be linked to healthy aging, extending healthspan.****************************Thanks to the >190,000 Ground Truths subscribers from every US state and 210 countries. Your subscription to these free essays and podcasts makes my work in putting them together worthwhile.If you found this interesting PLEASE share it!Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don’t hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. It enabled us to accept and support 47 summer interns in 2025! We aim to accept even more of the several thousand who will apply for summer 2026.Thank you Debbie Weil, Cynthia Brumfield, Sara Garcia, Harshi Peiris, Ph.D., Liane Moccia, and over 1,000 others for tuning into my live video with Dr. Jen Gunter! Join me for my next live video in the app. Get full access to Ground Truths at erictopol.substack.com/subscribe | 1h 00m 50s | ||||||
| 11/8/25 |  Dr. Susan Monarez—Former CDC Director, First Live Interview | Dr. Susan Monarez was the first CDC Director to be confirmed by the Senate and served from July 31, 2025 – August 27, 2025. Because she refused to give approval to new vaccine recommendations without ever seeing them or their evidence and firing scientists without cause, she was fired. In my view, she’s a hero for standing up for science and speaking truth to power.In her first live interview since leaving the CDC, we review her background. That includes growing up in rural Wisconsin and getting her college and PhD education at UW-Madison, the latter in microbiology and immunology. She then went on to 18 years of government service with an extensive portfolio of jobs and management at BARDA, the White House, ARPA-H, and others, before becoming Acting Director of the CDC in early 2025.We discussed the horrific CDC shooting on August 8th, days after she started. Then we reviewed a conversation that we had on August 19th in which she laid out her exciting vision for the future of CDC, emphasizing the goal of prevention (BTW, CDC stands for Centers for Disease Control and Prevention) and asked me to help as an advisor. At the time, she was well aware, with growing tension, that her tenure at CDC might be limited. I asked about her perspective for the jobs of 4,300 people at CDC who have been terminated, which account for more than 1/3rd of the workforce, no less the gutting of the budget.Then we got into what she learned from this ordeal and her plans for the future, which includes a very ambitious initiative: 90/90/2035. As you’ll see from our conversation, Dr. Monarez is exceptionally resilient and an optimist. She’s got lots to do in the years ahead to carry out her mission of promoting human health!Dr. Monarez just started a Substack The Road Best Traveled so you can follow her there. It was a real privilege for me to do this interview with her. In deep admiration of her willingness to not only take on the job of CDC Director in tough circumstances, her professionalism during testimony at the Senate committee hearing, her impressive yet unrealized vision for transforming the CDC, and refusing to cave to immense pressure from the HHS Secretary to move ahead with his agenda. Thank you Julie, Stephen B. Thomas, PhD, David Dansereau, MSPT, Dr. Sara Wolfson, Vau Geha, and >500 others for tuning into my live video with The Road Best Traveled! Thanks for being a Ground Truths subscriber! Please spread the word. Get full access to Ground Truths at erictopol.substack.com/subscribe | 54m 36s | ||||||
| 11/5/25 |  Seth Berkley & Eric Topol - Discuss Fair Doses Book | Get full access to Ground Truths at erictopol.substack.com/subscribe | 47m 19s | ||||||
| 10/1/25 |  Tom Frieden & Eric Topol - Discuss the Formula for Better Health Book | Get full access to Ground Truths at erictopol.substack.com/subscribe | 35m 02s | ||||||
| 9/14/25 | 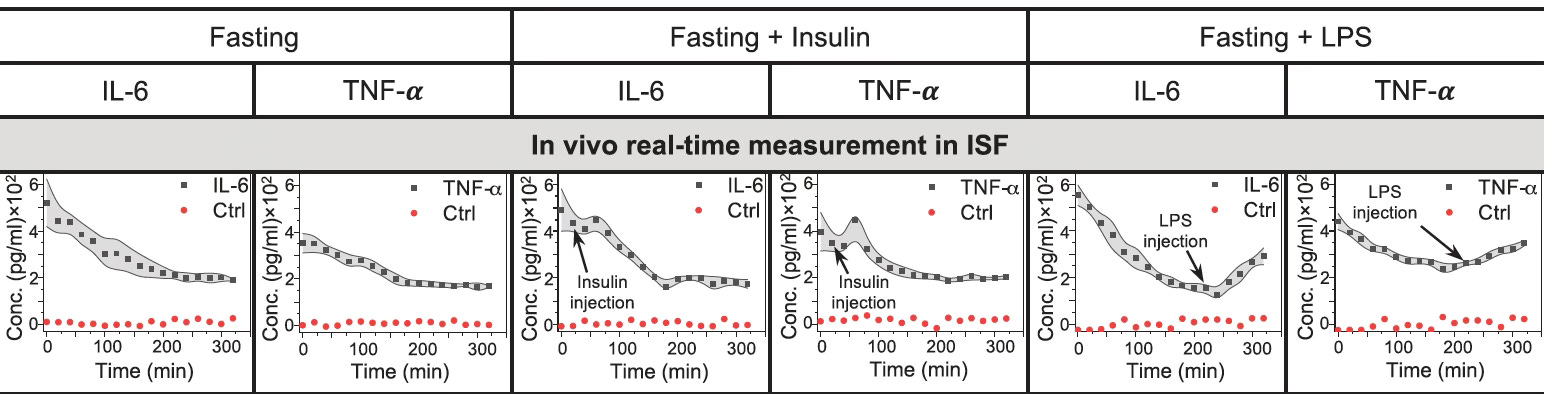 Shana Kelley: Biosensors to Track Proteins and Inflammation in Our Blood in Real Time | Prof Shana Kelley is the Neena Schwartz Professor of Chemistry and Biomedical Engineering at Northwestern University and President of the CZI Chicago Biohub, which brings together life scientists at Northwestern, University of Chicago, and U. Illinois Urbana Champaign. Her lab’s website provides recent publications in the 3 major areas of biomolecular sensors, rare and single cell analysis, and intracellular molecular delivery.You are undoubtedly familiar with wearable biosensors on the wrist and rings, and continuous glucose monitoring (CGM), all of which can transmit physiologic data in real time to your smartphone. What is different about Prof Kelley’s work is the ingenious way of continuously tracking any proteins in our blood via a sensor that could function just like CGM in the future (hair thin sensor applied just below the skin and data relayed to your smartphone). A proof-of-concept paper in Science showed how exquisitely sensitive such a sensor worked to track inflammation markers [interleukin-6 (IL-6) and tumor necrosis factor (TNF)] in the diabetic rat model. As seen. below, just the injection of insulin evoked inflammation, and introduction of lipopolysaccharide (LPS) did so markedly.This capability opens up the potential for monitoring body-wide inflammation in real time, but also extends to many other conditions such as autoimmune diseases, heart failure (e.g. continuous brain natriuetic peptide monitoring), and neurodegenerative diseases (with specific markers of neuroinflammation). This innovation represents a new dimension in individualized (precision) medicine.In our conversation, Shana takes us through the discovery of these unique bimolecular sensors that have no reagents, and use electricity to shake off the protein from DNA strands. And she maps out the path to clinical trials and commercialization in the next couple of years.Thank you Stephen B. Thomas, PhD, Linda Kemp, Lynn L, Pat Mumby PhD, David Hobson, and many others for tuning into my live video with Shana Kelley! Join me for my next live video in the app, along with posts on biomedical news and analysis.***********************************************************************Thanks you for your listening, reading and subscribing to Ground Truths.If you found this interesting PLEASE share it!That makes the work involved in putting these together especially worthwhile.All content on Ground Truths—its newsletters, analyses, and podcasts, are free, open-access.Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don't hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. It enabled us to accept and support 47 summer interns in 2025! Get full access to Ground Truths at erictopol.substack.com/subscribe | 31m 17s | ||||||
| 9/12/25 |  Charlotte Blease: Is A.I. Going to Remedy Medicine’s Problems? | Thank you Bruce Lanphear, Clyde Wilson, Tracy Dennis-Tiwary, Diego Pereyra, Dr Mike Hunter, and many others for tuning into my live video with Charlotte Blease! Join me for my next live video in the app.Whether A.I. will transform the practice of medicine in a positive way remains controversial. Health researcher Prof Charlotte Blease, on faculty at Uppsala University in Sweden and researcher at Harvard University, has written a new book —Dr. Bot—that critically assesses the unmet needs in healthcare and whether A.I. can fulfill them. She provides an optimistic viewpoint (see the subtitle), and our conversation probes whether that is justified. She has a substack, too, hereThanks for listening to Ground Truths. Through analytic essays and podcasts, I try to cover the important issues and discoveries in life science and medicine. If you have suggestions for topics I should get into, please pass them along. Get full access to Ground Truths at erictopol.substack.com/subscribe | 30m 37s | ||||||
| 9/8/25 |  Peter Hotez & Eric Topol - Discuss “Science Under Siege” book | Thank you Sara Garcia, Andrew O'Malley BSc PhD, Sam Hester, Julie, Stephen B. Thomas, PhD, and so many others for tuning into my live video with Peter Hotez! Join me for my next live video in the app.Peter Hotez and I discuss his new book, co-authored with Michael Mann, SCIENCE UNDER SEIGE, on the anti-science superstorm culminating from the climate crisis, the Covid pandemic, and a vast interconnected network that has waged a direct assault on scientific truth.During our conversation we trace history of priors in civilization, such as Lysenko and Stalinism in the last century. And acknowledge the future role of A.I. for promoting infinite disinformation. Beyond human suffering and direct health outcome consequences (such as Red Covid), the toll this is taking on the career of young scientists, universities, public health agencies, and loss of public trust are reviewed. The interdependent role of the media and the wellness industry is touched on.The book and our conversation puts forth a call to arms, potential solutions, including the need to move away from invisible scientists and political activism.Thanks for listening to Ground Truths podcasts and reading the analytic posts.In case you missed any, these are a few recent and related ones:Podcasts with Michael Osterholm and Sanjay Gupta on their new books—The Big One and It Doesn’t Have to Hurt, respectively.Next up is Charlotte Blease and her new book Dr. Bot on where we are headed with medical A.I.If you found this interesting PLEASE share it!That makes the work involved in putting these together especially worthwhile.All content on Ground Truths—its newsletters, analyses, and podcasts, are free, open-access.Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don't hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. Get full access to Ground Truths at erictopol.substack.com/subscribe | 53m 07s | ||||||
| 9/5/25 |  Sanjay Gupta & Eric Topol - Discuss “It Doesn’t Have to Hurt” book | Thank you Jose Bolanos MD, Dr. Zeest Khan, Lawrence Toole, Julie, Stephen B. Thomas, PhD, and many others for tuning into my live video with Dr. Sanjay Gupta. Join me for my next live video in the app.A Brief Summary of Our ConservationWe discussed the new understanding and approach to chronic pain, which affects nearly 1 in 4 adults. Dr. Gupta gets personal telling the story of his wife, Rebecca, who has an autoimmune disease and at one point he had to carry her up stairs. He also tells the story of his mother who had a back injury and didn’t want to live because of the pain. How his family members got relief is illuminating.Our whole understanding and approach to pain has changed, with the acronym change from RICE to MEAT.A newly approved drug Suzetrigine (Journavx) exploits the sodium channel gene mutation initially discovered via a family of fire walkers. It’s the first new pain medicine approved for more than 2 decades. Many other new non-opioid treatments are reviewed, no less lifestyle changes (anti-inflammatory diet and sleep), and acupuncture.Sanjay’s research over the past few years has led to a video special on CNN with the same title as the book, set to air 9 PM EST Sunday. If you know someone suffering chronic pain, please share the post. Get full access to Ground Truths at erictopol.substack.com/subscribe | 22m 06s | ||||||
| 9/3/25 |  Mike Osterholm & Eric Topol - Discuss “The Big One” book | Get full access to Ground Truths at erictopol.substack.com/subscribe | 36m 12s | ||||||
| 8/17/25 |  Bruce Lanphear: Chronic Lead Exposure, a Risk Factor for Heart Disease | This is a hybrid heart disease risk factor post of a podcast with Prof Bruce Lanphear on lead and a piece I was asked to write for the Washington Post on risk factors for heart disease.First, the podcast. You may have thought the problem with lead exposure was circumscribed to children, but it’s a much bigger issue than that. I’ll concentrate on the exposure risk to adults in this interview, including the lead-estrogen hypothesis. Bruce has been working on the subject of lead exposure for more than 30 years. Let me emphasize that the problem is not going away, as highlighted in a recent New England Journal of Medicine piece on lead contamination in Milwaukee schools, “The Latest Episode in an Ongoing Toxic Pandemic.”Transcript with links to the audio and citationsEric Topol (00:05):Well, hello. This is Eric Topol with Ground Truths, and I'm very delighted to welcome Professor Bruce Lanphear from Simon Fraser University in British Columbia for a very interesting topic, and that's about lead exposure. We tend to think about lead poisoning with the Flint, Michigan, but there's a lot more to this story. So welcome, Bruce.Bruce Lanphear (00:32):Thank you, Eric. It's great to be here.Eric Topol (00:33):Yeah. So you had a New England Journal of Medicine (NEJM) Review in October last year, which was probably a wake up to me, and I'm sure to many others. We'll link to that, where you reviewed the whole topic, the title is called Lead Poisoning. But of course it's not just about a big dose, but rather chronic exposure. So maybe you could give us a bit of an overview of that review that you wrote for NEJM.Bruce Lanphear (01:05):Yeah, so we really focused on the things where we feel like there's a definitive link. Things like lead and diminished IQ in children, lead and coronary heart disease, lead and chronic renal disease. As you mentioned, we've typically thought of lead as sort of the overt lead poisoning where somebody becomes acutely ill. But over the past century what we've learned is that lead is one of those toxic chemicals where it's the chronic wear and tear on our bodies that catches up and it's at the root of many of these chronic diseases that are causing problems today.Eric Topol (01:43):Yeah, it's pretty striking. The one that grabbed me and kind of almost fell out of my chair was that in 2019 when I guess the most recent data there is 5.5 million cardiovascular deaths ascribed to relatively low levels, or I guess there is no safe level of lead exposure, that's really striking. That's a lot of people dying from something that cardiology and medical community is not really aware of. And there's a figure 3 [BELOW] that we will also show in the transcript, where you show the level where you start to see a takeoff. It starts very low and by 50 μg/liter, you're seeing a twofold risk and there's no threshold, it keeps going up. How many of us do you think are exposed to that type of level as adults, Bruce?Bruce Lanphear (02:39):Well, as adults, if we go back in time, all of us. If you go back to the 1970s when lead was still in gasoline, the median blood lead level of Americans was about 13 to 15 µg/dL. So we've all been exposed historically to those levels, and part of the reason we've begun to see a striking decline in coronary heart disease, which peaked in 1968. And by 1978, there was a 20% decline, 190,000 more people were alive than expected. So even in that first decade, there was this striking decline in coronary heart disease. And so, in addition to the prospective studies that have found this link between an increase in lead exposure and death from cardiovascular disease and more specifically coronary heart disease. We can look back in time and see how the decline in leaded gasoline led to a decline in heart disease and hypertension.Eric Topol (03:41):Yeah, but it looks like it's still a problem. And you have a phenomenal graph that's encouraging, where you see this 95% reduction in the lead exposure from the 1970s. And as you said, the factors that can be ascribed to like getting rid of lead from gasoline and others. But what is troubling is that we still have a lot of people that this could be a problem. Now, one of the things that was fascinating is that you get into that herbal supplements could be a risk factor. That we don't do screening, of course, should we do screening? And there's certain people that particularly that you consider at high risk that should get screened. So I wasn't aware, I mean the one type of supplements that you zoomed in on, how do you say it? Ayurvedic?Supplements With LeadBruce Lanphear (04:39):Oh yeah. So this is Ayurvedic medicine and in fact, I just was on a Zoom call three weeks ago with a husband and wife who live in India. The young woman had taken Ayurvedic medicine and because of that, her blood lead levels increased to 70 µg/dL, and several months later she was pregnant, and she was trying to figure out what to do with this. Ayurvedic medicine is not well regulated. And so, that's one of the most important sources when we think about India, for example. And I think you pointed out a really important thing is number one, we don't know that there's any safe level even though blood lead levels in the United States and Europe, for example, have come down by over 95%. The levels that we're exposed to and especially the levels in our bones are 10 to 100 times higher than our pre-industrial ancestors.Bruce Lanphear (05:36):So we haven't yet reached those levels that our ancestors were exposed to. Are there effects at even lower and lower levels? Everything would suggest, we should assume that there is, but we don't know down below, let's say one microgram per deciliter or that's the equivalent of 10 parts per billion of lead and blood. What we also know though is when leaded gasoline was restricted in the United States and Canada and elsewhere, the companies turned to the industrializing countries and started to market it there. And so, we saw first the epidemic of coronary heart disease in the United States, Canada, Europe. Then that's come down over the past 50 years. At the same time, it was rising in low to middle income countries. So today over 95% of the burden of disease from lead including heart disease is found in industrializing countries.Eric Topol (06:34):Right. Now, it's pretty striking, of course. Is it true that airlines fuel is still with lead today?Bruce Lanphear (06:45):Well, not commercial airlines. It's going to be a small single piston aircraft. So for example, when we did a study down around the Santa Clara County Airport, Reid-Hillview, and we can see that the children who live within a half mile of the airport had blood lead levels about 10% higher than children that live further away. And the children who live downwind, 25% higher still. Now, nobody's mapped out the health effects, but one of the things that's particularly troubling about emissions from small aircraft is that the particle size of lead is extraordinarily small, and we know how nanoparticles because they have larger surface area can be more problematic. They also can probably go straight up into the brain or across the pulmonary tissues, and so those small particles we should be particularly worried about. But it's been such a long journey to try to figure out how to get that out of aircraft. It's a problem. The EPA recognized it. They said it's an endangerment, but the industry is still pushing back.Eric Topol (07:55):Yeah, I mean, it's interesting that we still have these problems, and I am going to in a minute ask you what we can do to just eradicate lead as much as possible, but we're not there yet. But one study that seemed to be hard to believe that you cited in the review. A year after a ban leaded fuel in NASCAR races, mortality from coronary heart disease declined significantly in communities near racetracks. Can you talk about that one because it's a little bit like the one you just mentioned with the airports?Bruce Lanphear (08:30):Yeah. Now that study particularly, this was by Alex Hollingsworth, was particularly looking at people over 65. And we're working on a follow-up study that will look at people below 65, but it was quite striking. When NASCAR took lead out of their fuel, he compared the rates of coronary heart disease of people that live nearby compared to a control group populations that live further away. And he did see a pretty striking reduction. One of the things we also want to look at in our follow-up is how quickly does that risk begin to taper off? That's going to be really important in terms of trying to develop a strategy around preventing lead poisoning. How quickly do we expect to see it fall? I think it's probably going to be within 12 to 24 months that we'll see benefits.Eric Topol (09:20):That's interesting because as you show in a really nice graphic in adults, which are the people who would be listening to this podcast. Of course, they ought to be concerned too about children and all and reproductive health. But the point about the skeleton, 95% of the lead is there and the main organs, which we haven't mentioned the kidney and the kidney injury that occurs no less the cardiovascular, the blood pressure elevation. So these are really, and you mentioned not necessarily highlighted in that graphic, but potential cognitive hit as well. You also wrote about how people who have symptoms of abdominal pain, memory impairment, and high blood pressure that's unexplained, maybe they should get a blood level screening. I assume those are easy to get, right?Bruce Lanphear (10:17):Oh yeah, absolutely. You can get those in any hospital, any clinic across the country. We're still struggling with having those available where it's most needed in the industrializing countries, but certainly available here. Now, we don't expect that for most people who have those symptoms, lead poisoning is going to be the cause, right. It'd still be unusual unless you work in an industry, for example, smelting batteries to recycle them. We don't expect it to be real common, and we're not even sure, Eric, whether we should be doing widespread screening. If I looked at this as a population scientist, the real focus should be on identifying the sources. We mostly know where those are here and radically moving it down. Getting rid of the lead service lines, which was such a big part of what President Biden was doing, and it was perfect. For every dollar invested to reduce lead exposure from those lead service lines. Ronnie Levin at Harvard said there'd be a 35-fold return in cost, benefits really, and this has always been true, that reducing lead exposure throughout the past 40 years has always been shown to be amazingly cost beneficial. The problem is operating within a free market health system, even though there's tremendous social benefits, that benefit isn't going to be monetized or privatized. And so, who's going to make those decisions? We hope our government is, but that doesn't always play out.Eric Topol (11:52):Well. What's interesting is, as opposed to the problems we have today that are prominent such as the microplastic, nanoplastics, the air pollution, the forever chemicals, that just keep getting worse, I mean, they are just cumulative. This one, there was tremendous improvement, but it’s still not enough. And I guess you're zooming in on the lead lines. That'd be the most important thing to work on today. Another thing that has come up, there's been trials, as you may I'm sure, because all over this field of chelation, there's a trial that was run by the NIH, supported by NH that looked at chelation to prevent coronary disease. Is there any evidence that people who have a problem with lead would benefit from chelation therapy?Bruce Lanphear (12:44):Well, there's two major studies that have been done, and Tony Lamas was in charge of both of them. The first one Trial to Assess Chelation Therapy (TACT) study, it was a randomized controlled trial, not intended specifically to focus on lead, but rather it was to look at sort of this alternative therapy. They found significant benefits about an 18% reduction in subsequent cardiac events. That led to a second study that was just published last year, and it was focused on people who had diabetes. They saw some benefit, but it wasn't significant. So whether that's because there wasn't enough variability and exposure, it's not entirely clear, but we've seen this with lead in IQ deficits in kids where we can show that we can reduce blood lead levels. But ultimately what tends to happen is once you've taken lead out of the blood, some of it's released again from the bone, but you still have all that lead in the bone that's there. You get some of it out, but you're not going to get the bulk of it out.The Lead-Estrogen HypothesisEric Topol (13:47):Right. It's a reservoir that's hard to reckon with. Yeah. Now another thing, you have a Substack that is called Plagues, Pollution & Poverty, and you wrote a really provocative piece in that earlier and April called How Estrogen Keeps Lead - and Heart Attacks - in Check, and basically you got into the lead estrogen hypothesis.Eric Topol (14:10):Can you enlighten us about that?Bruce Lanphear (14:12):Yeah. A lot of the seminal work in this area was done by Ellen Silbergeld, who's a brilliant and somewhat peculiar toxicologist and Ellen for years, I focused on childhood lead exposure, and for years Ellen would tell me, almost demolish me for not studying adults. And because she had found back in 1988 that as women go into menopause, their blood lead levels spike increased by about 30%, and that's where most of our lead is stored is in our bone. And so, as I was thinking about this, it all became clear because blood lead levels in boys and girls is about the same. It's comparable up until menarche, and then girls young women's blood leads fall by about 20%. And they stay 20% lower throughout the reproductive years until menopause. And especially during those first few years around menopause, perimenopause, you see fairly striking increases in the weakening of the bone and blood lead levels.Bruce Lanphear (15:19):So that might very well help to explain why estrogen is protected, because what happens is throughout the reproductive life, women are losing a little bit of lead every month. And estrogen is at its lowest during that time, and that's going to be when blood lead is at its highest because estrogen pushes lead into the bone. Not only that, women lose lead into the developing fetus when they're pregnant. So what Ellen found is that there was less of a spike around menopause for the women that had three or four pregnancies because they had offloaded that into their babies. So all of this, if you put it together, and this is of course in a very short note of it, you can see that lead increases dyslipidemia, it leads to tears in the endothelium of the arterial wall, it's going to increase thrombosis. All of these things that we think of as the classic atherosclerosis. Well, what estrogen does is the opposite of those. It decreases dyslipidemia, it repairs the arterial endothelial wall. So how much of it is that estrogen is protective, and how much is it that it's moving lead out of the system, making it less biologically available?Eric Topol (16:46):Yeah, I know. It's really interesting. Quite provocative. Should be followed up on, for sure. Just getting to you, you're a physician and epidemiologist, MD MPH, and you have spent your career on this sort of thing, right? I mean, is your middle name lead or what do you work on all the time?Bruce Lanphear (17:09):Yeah, I've been doing this for about 30 years, and one of my mentors, Herb Needleman spent 40 years of his career on it. And in some ways, Eric, it seems to me particularly in these very difficult entrenched problems like lead, we don't have any pharmaceutical company reaching out to us to promote what we do. We've got industry trying to squash what we do.Bruce Lanphear (17:35):It really does take a career to really make a dent in this stuff. And in a way, you can look at my trajectory and it is really following up on what Herb Needleman did and what Clare Patterson did, and that was finding the effects at lower and lower levels. Because what we do with lead and most other toxic chemicals, the ones that don't cause cancer, is we assume that there's a safe level or threshold until we prove otherwise. And yet when you look at the evidence, whether it's about asbestos and mesothelioma, air pollution and cardiovascular mortality, lead and cardiovascular mortality, benzene and leukemia, none of those exhibit a threshold. In some cases, the risks are steepest proportionately at the lowest measurable levels, and that really raises some tremendous challenges, right? Because how are we going to bring air pollution or lead down to zero? But at the same time, it also provides these tremendous opportunities because we know that they're causing disease. We know what the sources are. If we could only bring about the political will to address them, we could prevent a lot of death, disease, and disability. I mean, about 20% of deaths around the world every year are from air pollution, lead, and other toxic chemicals, and yet the amount of money we invest in them is just paltry compared to what we invest in other things. Which is not to pit one against the other, but it's to say we haven't invested enough in these.Eric Topol (19:14):No, absolutely. I think your point, just to make sure that it's clear, is that even at low levels, this is of course where most of the population exposure would be, and that's why that's so incriminating. Now, one of the things I just want to end up with is that we know that these are tiny, tiny particles of lead, and then the question is how they can synergize and find particulate matter of air pollution in the nanoplastic, microplastic story and binding to forever chemicals, PFAS. How do you process all that? Because it's not just a single hit here, it's also the fact that there's ability to have binding to the other environmental toxins that are not going away.Bruce Lanphear (20:10):That's right. And in a way, when we talk about lead playing this tremendous role in the rise and decline of coronary heart disease, we can't entirely separate it out, for example, from air pollution or cigarette smoke for that matter, nor plastic. So for example, with air pollution, if we look at air pollution over the past century, up until the 1980s, even into the 1990s, it was leaded, right? So you couldn't separate them. If you look at cigarette smoke, cigarette tobacco in the 1940s and 1950s was grown in fields where they used lead arsenic as an insecticide. So smokers even today have blood lead levels that are 20% higher than non-smokers, and people who are not smokers but exposed to secondhand smoke have blood lead levels 20% higher than non-smokers who aren't exposed to secondhand smoke. So in a way, we should try to tease apart these differences, but it's going to be really challenging. In a way we can almost think about them as a spectrum of exposures. Now with plastics, you can really think of plastics as a form of pollution because it's not just one thing. There's all these additives, whether it's the PFAS chemicals or lead, which is used as a stabilizer. And so, all of them really are kind of integrated into each other, which again, maybe there's some opportunity there if we really were ready to tackle.Eric Topol (21:40):And interestingly, just yesterday, it was announced by the current administration that they're stopping all the prior efforts on the forever chemicals that were initiated in the water supply. And I mean, if there's one takeaway from our discussion, it's that we have to get all over this and we're not paying enough attention to our environmental exposures. You've really highlighted spotlighted the lead story. And obviously there are others that are, instead of getting somewhat better, they're actually going in the opposite direction. And they're all tied together that’s what is so striking here, and they all do many bad things to our bodies. So I don't know how, I'm obviously really interested in promoting healthy aging, and unless we get on this, we're chasing our tails, right?Bruce Lanphear (22:31):Well, I think that's right, Eric. And I was reading the tips that you'd written about in preparation for your book release, and you focused understandably on what each of us can do, how we can modify our own lifestyles. We almost need six tips about what our government should do in order to make it harder for us to become sick, or to encourage those healthy behaviors that you talked about. That's a big part of it as well. One of the things we're celebrating the hundredth anniversary. This is not really something to celebrate, but we are. The hundredth anniversary of the addition of tetraethyl lead to gasoline. And one of the key things about that addition, there was this debate because when it was being manufactured, 80% of the workers at a plant in New Jersey suffered from severe lead poisoning, and five died, and it was enough that New York City, Philadelphia and New Jersey banned tetraethyl lead.Bruce Lanphear (23:31):Then there was this convening by the US Surgeon General to determine whether it was safe to add tetraethyl lead to gasoline. One scientist, Yandell Henderson said, absolutely not. You're going to create a scourge worse than tuberculosis with slow lead poisoning and hardening of your arteries. Robert Kehoe, who represented the industry said, we know lead is toxic, but until you've shown that it's toxic when added to gasoline, you have no right to prohibit us from using it. So that is now known as the Kehoe rule, and it's relevant not only for lead, but for PFAS, for air pollution, for all these other things, because what it set as a precedent, until you've shown that these chemicals or pollution is toxic when used in commerce, you have no right to prohibit industry from using it. And that's the fix we're in.Eric Topol (24:27):Well, it sounds too much like the tobacco story and so many other things that were missed opportunities to promote public health. Now, is Canada doing any better than us on this stuff?Bruce Lanphear (24:40):In some ways, but not in others. And one of the interesting thing is we don't have standards, we have guidelines. And amazingly, the cities generally try to conform to those guidance levels. With water lead, we're down to five parts per billion. The US is sticking around with ten parts per billion, but it's not even really very, it's not enforced very well. So we are doing better in some ways, not so good in other ways. The European Union, generally speaking, is doing much better than North America.Eric Topol (25:15):Yeah, well, it doesn't look very encouraging at the moment, but hopefully someday we'll get there. Bruce, this has been a really fascinating discussion. I think we all should be thankful to you for dedicating your career to a topic that a lot of us are not up on, and you hopefully are getting us all into a state of awareness. And congratulations on that review, which was masterful and keep up the great work. Thank you.Bruce Lanphear (25:42):Thank you, Eric. I appreciate it.________________________________________________My Recommendations for Preventing Heart Disease (Markedly Truncated from Text and Graphics Provided in SUPER AGERS)Recently the Washington Post asked me for a listicle of 10 ways to prevent heart disease. I generally avoid making such lists but many people have de-subscribed to this newspaper, never subscribed, or missed the post, so here it is with links to citations:Guest column by Eric Topol, MDThe buildup of cholesterol and other substances in the wall of our arteries, known as atherosclerosis, is common. It can lead to severe plaques that narrow the artery and limit blood flow, or to a crack in the artery wall that can trigger blood clot formation, resulting in a heart attack.While we’ve seen some major advances in treating heart disease, it remains the leading killer in the United States, even though about 80 percent of cases are considered preventable. There are evidence-based steps you can take to stave it off. As a cardiologist, here’s what I recommend to my patients.1. Do both aerobic and resistance exerciseThis is considered the single most effective medical intervention to protect against atherosclerosis and promote healthy aging. Physical activity lowers inflammation in the body. Evidence has shown that both aerobic and strength training forms of exercise are important. But only 1 in 4 Americans meet the two activity guidelines from the American Heart Association: aerobic exercise of 150 minutes per week of at least moderate physical activity, such as walking, bicycling on level ground, dancing or gardening, and strength training for at least two sessions per week, which typically translates to 60 minutes weekly.The protective benefit of exercise is seen with even relatively low levels of activity, such as around 2,500 steps per day (via sustained physical activity, not starting and stopping), and generally increases proportionately with more activity. It used to be thought that people who exercise only on the weekend — known as “weekend warriors” — put themselves in danger, but recent data shows the benefits of exercise can be derived from weekend-only workouts, too.2. Follow an anti-inflammatory dietA predominantly plant-based diet — high in fiber and rich in vegetables, fruits and whole grains, as seen with the Mediterranean diet — has considerable evidence from large-scale observational and randomized trials for reducing body-wide inflammation and improving cardiovascular outcomes.Foods rich in omega-3 fatty acids, such as salmon, also form part of a diet that suppresses inflammation. On the other hand, red meat and ultra-processed foods are pro-inflammatory, and you should limit your consumption. High protein intake of more than 1.4 grams per kilogram of body weight per day — around 95 grams for someone who is 150 pounds — has also been linked to promoting inflammation and to atherosclerosis in experimental models. That is particularly related to animal-based proteins and the role of leucine, an essential amino acid that is obtained only by diet.3. Maintain a healthy weightBeing overweight or obese indicates an excess of white adipose tissue. This kind of tissue can increase the risk of heart disease because it stores fat cells, known as adipocytes, which release substances that contribute to inflammation.In studies, we’ve seen that glucagon-like peptide (GLP-1) drugs can reduce inflammation with weight loss, and a significant reduction of heart attacks and strokes among high-risk patients treated for obesity. Lean body weight also helps protect against atrial fibrillation, the most common heart rhythm abnormality.4. Know and avoid metabolic syndrome and prediabetesTied into obesity, in part, is the problem of insulin resistance and metabolic syndrome. Two out of three people with obesity have this syndrome, which is defined as having three out of five features: high fasting blood glucose, high fasting triglycerides, high blood pressure, low high-density lipoprotein (HDL) and central adiposity (waist circumference of more than 40 inches in men, 35 inches in women).Metabolic syndrome is also present in a high proportion of people without obesity, about 50 million Americans. Prediabetes often overlaps with it. Prediabetes is defined as a hemoglobin A1c (a measure of how much glucose is stuck to your red blood cells) between 5.7 and 6.4 percent, or a fasting glucose between 100 and 125 milligrams per deciliter.Both metabolic syndrome and prediabetes carry an increased risk of heart disease and can be prevented — and countered — by weight loss, exercise and an optimal diet.As the glucagon-like peptide drug family moves to pills and less expense in the future, these medications may prove helpful for reducing risk in people with metabolic syndrome and prediabetes. For those with Type 2 diabetes, the goal is optimizing glucose management and maximal attention to lifestyle factors.5. Keep your blood pressure in a healthy rangeHypertension is an important risk factor for heart disease and is exceptionally common as we age. The optimal blood pressure is 120/80 mm Hg or lower. But with aging, there is often an elevation of systolic blood pressure to about 130 mm Hg, related to stiffening of arteries. While common, it is still considered elevated.Ideally, everyone should monitor their blood pressure with a home device to make sure they haven’t developed hypertension. A mild abnormality of blood pressure will typically improve with lifestyle changes, but more substantial elevations will probably require medications.6. Find out your genetic riskWe now have the means of determining your genetic risk of coronary artery disease with what is known as a polygenic risk score, derived from a gene chip. The term polygenic refers to hundreds of DNA variants in the genome that are linked to risk of heart disease. This is very different from a family history, because we’re a product of both our mother’s and father’s genomes, and the way the DNA variants come together in each of us can vary considerably for combinations of variants.That means you could have high or low risk for heart disease that is different from your familial pattern. People with a high polygenic risk score benefit the most from medications to lower cholesterol, such as statins. A polygenic risk score can be obtained from a number of commercial companies, though it isn’t typically covered by insurance.I don’t recommend getting a calcium score of your coronary arteries via a computed tomography (CT) scan. This test is overused and often induces overwhelming anxiety in patients with a high calcium score but without symptoms or bona fide risk. If you have symptoms suggestive of coronary artery disease, such as chest discomfort with exercise, then a CT angiogram may be helpful to map the coronary arteries. It is much more informative than a calcium score.7. Check your blood lipidsThe main lipid abnormality that requires attention is low-density cholesterol (LDL), which is often high and for people with increased risk of heart disease should certainly be addressed. While lifestyle improvements can help, significant elevation typically requires medications such as a statin; ezetimibe; bempedoic acid; or injectables such as evolocumab (Repatha), alirocumab (Praluent) or inclisiran (Leqvio). The higher the risk, the more aggressive LDL lowering may be considered.It should be noted that the use of potent statins, such as rosuvastatin or atorvastatin, especially at high doses, is linked to inducing glucose intolerance and risk of Type 2 diabetes. While this is not a common side effect, it requires attention since it is often missed from lack of awareness.A low high-density lipoprotein (HDL) cholesterol often responds to weight loss and exercise. We used to think that high HDL was indicative of “good cholesterol,” but more recent evidence suggests that is not the case and it may reflect increased risk when very high.To get a comprehensive assessment of risk via your blood lipids, it’s important to get the apolipoprotein B (apoB) test at least once because about 20 percent of people have normal LDL and a high apoB.Like low HDL, high fasting triglycerides may indicate insulin resistance as part of the metabolic syndrome and will often respond to lifestyle factors.The lipoprotein known as Lp(a) should also be assessed at least once because it indicates risk when elevated. The good news is scientists are on the cusp of finally having medications to lower it, with five different drugs in late-stage clinical trials.8. Reduce exposure to environmental pollutantsIn recent years, we’ve learned a lot about the substantial pro-inflammatory effects of air pollution, microplastics and forever chemicals, all of which have been linked to a higher risk of heart disease. In one study, microplastics or nanoplastics in the artery wall were found in about 60 percent of more than 300 people. Researchers found a vicious inflammatory response around the plastics, and a four- to fivefold risk of heart attacks or strokes during three years of follow-up.While we need policy changes to address these toxic substances in the environment, risk can be reduced by paying attention to air and water quality using filtration or purification devices, less use of plastic water bottles and plastic storage, and, in general, being much more aware and wary of our pervasive use of plastics.9. Don’t smoke This point, it should be well known that cigarette smoking is a potent risk factor for coronary artery disease and should be completely avoided.10. Get Good SleepAlthough we tend to connect sleep health with brain and cognitive function, there’s evidence that sleep regularity and quality are associated with less risk of heart disease. Regularity means adhering to a routine schedule as much as possible, and its benefit may be due to our body’s preference for maintaining its circadian rhythm. Sleep quality — meaning with fewer interruptions — and maximal deep sleep can be tracked with smartwatches, fitness bands, rings or mattress sensors.Sleep apnea, when breathing stops and starts during sleep, is fairly common and often unsuspected. So if you’re having trouble sleeping or you snore loudly, talk to your doctor about ruling out the condition. Testing for sleep apnea can involve checking for good oxygen saturation throughout one’s sleep. That can be done through a sleep study or at home using rings or smartwatches that include oxygen saturation in their sensors and body movement algorithms that pick up disturbed breathing.Eric Topol, MD, is a cardiologist, professor and executive vice president of Scripps Research in San Diego. He is the author of “Super Agers: An Evidence-Based Approach to Longevity” and the author of Ground Truths on Substack.*********************°°°°°°°°°°°°°°°°°°°°Thanks to many of you Ground Truths subscribers who helped put SUPER AGERS on the NYT bestseller list for 4 weeks.Here are 2 recent, informative, and fun conversations I had on the topicMichael Shermer, The SkepticRuss Roberts, EconTalk I’m also very appreciative for your reading and subscribing to Ground Truths.If you found this interesting PLEASE share it!That makes the work involved in putting these together especially worthwhile.All content on Ground Truths—its newsletters, analyses, and podcasts, are free, open-access.Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don't hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past three years. Just a week ago we just had nearly 50 interns (high school, college and medical students) present posters of the work they did over the summer and it was exhilarating! Some photos below Get full access to Ground Truths at erictopol.substack.com/subscribe | 25m 53s | ||||||
| 7/13/25 |  Owen Tripp: Why Can't I Find and Get to the Right Doctor? | Eric Topol (00:06):Hello, this is Eric Topol from Ground Truths, and I'm delighted to welcome Owen Tripp, who is a CEO of Included Health. And Owen, I'd like to start off if you would, with the story from 2016, because really what I'm interested in is patients and how to get the right doctor. So can you tell us about when you lost your hearing in your right ear back, what, nine years ago or so?Owen Tripp (00:38):Yeah, it's amazing to say nine years, Eric, but obviously as your listeners will soon understand a pretty vivid memory in my past. So I had been working as I do and noticed a loss of hearing in my right ear. I had never experienced any hearing loss before, and I went twice actually to a sort of national primary care chain that now owned by Amazon actually. And they described it as eustachian tube dysfunction, which is a pretty benign common thing that basically meant that my tubes were blocked and that I needed to have some drainage. They recommended Sudafed to no effect. And it was only a couple weeks later where I was walking some of the senior medical team at my company down to the San Francisco Giants game. And I was describing this experience of hearing loss and I said I was also losing a little bit of sensation in the right side of my face. And they said, that is not eustachian tube dysfunction. And well, I can let the story unfold from there. But basically my colleagues helped me quickly put together a plan to get this properly diagnosed and treated. The underlying condition is called vestibular schwannoma, even more commonly known as an acoustic neuroma. So a pretty rare benign brain tumor that exists on the vestibular nerve, and it would've cost my life had it not been treated.Eric Topol (02:28):So from what I gather, you saw an ENT physician, but that ENT physician was not really well versed in this condition, which is I guess a bit surprising. And then eventually you got to the right ENT physician in San Francisco. Is that right?Owen Tripp (02:49):Well, the first doctor was probably an internal medicine doctor, and I think it's fair to say that he had probably not seen many, if any cases. By the time I reached an ENT, they were interested in working me up for what's known as sudden sensorineural hearing loss (SSHL), which is basically a fancy term for you lose hearing for a variety of possible pathologies and reasons, but you go through a process of differential diagnosis to understand what's actually going on. By the time that I reached that ENT, the audio tests had showed that I had significant hearing loss in my right ear. And what an MRI would confirm was this mass that I just described to you, which was quite large. It was already about a centimeter large and growing into the inner ear canal.Eric Topol (03:49):Yeah, so I read that your Stanford brain scan suggested it was about size of a plum and that you then got the call that you had this mass in your brainstem tumor. So obviously that's a delicate operation to undergo. So the first thing was getting a diagnosis and then the next thing was getting the right surgeon to work on your brain to resect this. So how did you figure out who was the right person? Because there's only a few thousand of these operations done every year, as I understand.Owen Tripp (04:27):That's exactly right. Yeah, very few. And without putting your listeners to sleep too early in our discussion, what I'll say is that there are a lot of ways that you can actually do this. There are very few cases, any approach really requires either shrinking or removing that tumor entirely. My size of tumor meant it was really only going to be a surgical approach, and there I had to decide amongst multiple potential approaches. And this is what's interesting, Eric, you started saying you wanted to talk about the patient experience. You have to understand that I'm somebody, while not a doctor, I lead a very large healthcare company. We provide millions of visits and services per year on very complex medical diagnoses down to more standard day-to-day fare. And so, being in the world of medical complexity was not daunting on the basics, but then I'm the patient and now I have to make a surgical treatment decision amongst many possible choices, and I was able to get multiple opinions.Owen Tripp (05:42):I got an opinion from the House clinic, which is closer to you in LA. This is really the place where they invented the surgical approach to treating these things. I also got an approach shared with me from the Mayo Clinic and one from UCSF and one from Stanford, and ultimately, I picked the Stanford team. And these are fascinating and delicate structures as you know that you're dealing with in the brain, but the surgery is a long surgery performed by multiple surgeons. It's such an exhausting surgery that as you're sort of peeling away that tumor that you need relief. And so, after a 13 hour surgery, multiple nights in the hospital and some significant training to learn how to walk and move and not lose my balance, I am as you see me today, but it was possible under one of the surgical approaches that I would've lost the use of the right side of my face, which obviously was not an option given what I given what I do.Eric Topol (06:51):Yeah, well, I know there had to be a tough rehab and so glad that you recovered well, and I guess you still don't have hearing in that one ear, right?Owen Tripp:That's right.Eric Topol:But otherwise, you're walking well, and you've completely recovered from what could have been a very disastrous type of, not just the tumor itself, but also the way it would be operated on. 13 hours is a long time to be in the operating room as a patient.Owen Tripp (07:22):You've got a whole team in there. You've got people testing nerve function, you've got people obviously managing the anesthesiology, which is sufficiently complex given what's involved. You've got a specialized ENT called a neurotologist. You've got the neurosurgeon who creates access. So it's quite a team that does these things.Eric Topol (07:40):Yeah, wow. Now, the reason I wanted to delve into this from your past is because I get a call or email or whatever contact every week at least one, is can you help me find the right doctor for such and such? And this has been going on throughout my career. I mean, when I was back in 20 years ago at Cleveland Clinic, the people on the board, I said, well, I wrote about it in one of my books. Why did you become a trustee on the board? And he said, so I could get access to the right doctor. And so, this is amazing. We live in an information era supposedly where people can get information about this being the most precious part, which is they want to get the right diagnosis, they want to get the right treatment or prevention, whatever, and they can't get it. And I'm finding this just extraordinary given that we can do deep research through several different AI models and get reports generated on whatever you want, but you can't get the right doctor. So now let's go over to what you're working on. This company Included Health. When did you start that?Owen Tripp (08:59):Well, I started the company that was known as Grand Rounds in 2011. And Grand Rounds still to this day, we've rebranded as Included Health had a very simple but powerful idea, one you just obliquely referred to, which is if we get people to higher quality medicine by helping them find the right level and quality of care, that two good things would happen. One, the sort of obvious one, patients would get better, they'd move on with their lives, they'd return to health. But two and critically that we would actually help the system overall with the cost burden of unnecessary, inappropriate and low quality care because the coda to the example you gave of people calling you looking for a physician referral, and you and I both know this, my guess is you've probably had to clean plenty of it up in your career is if you go to the wrong doctor, you don't get out of the problem. The problem just persists. And that patient is likely to bounce around like a ping pong ball until they find what they actually need. And that costs the payers of healthcare in this country a lot of money. So I started the company in 2011 to try to solve that problem.Eric Topol (10:14):Yeah, one example, a patient of mine who I've looked after for some 35 years contacted me and said, a very close friend of mine lives in the Palm Springs region and he has this horrible skin condition and he's tortured and he's been to six centers, UCSF, Stanford, Oregon Health Science, Eisenhower, UCLA, and he had a full workup and he can't sleep because he's itching all the time. His whole skin is exfoliating and cellulitis and he had biopsies everywhere. He’s put on all kinds of drugs, monoclonal antibodies. And I said to this patient of mine I said, I don't know, this is way out of my area. I checked at Scripps and turns out there was this kind of the Columbo of dermatology, he can solve any mystery. And the patient went to see him, and he was diagnosed within about a minute that he had scabies, and he was treated and completely recovered after having thousands and thousands of dollars of all these workups at these leading medical centers that you would expect could make a diagnosis of scabies.Owen Tripp (11:38):That’s a pretty common diagnosis.Eric Topol (11:40):Yeah. I mean you might expect it more in somebody who was homeless perhaps, but that doesn't mean it can't happen in anyone. And within the first few minutes he did a scrape and showed the patient under the microscope and made a definitive diagnosis and the patient to this day is still trying to pay all his bills for all these biopsies and drugs and whatnot, and very upset that he went through all this for over a year and he thought he wanted to die, it was so bad. Now, I had never heard of Included Health and you have now links with a third of the Fortune 100 companies. So what do you do with these companies?Owen Tripp (12:22):Yeah, it's pretty cool. These companies, so very large organizations like Walmart and JPMorgan Chase and the rest of the big pioneers of American industry and business put us in as a benefit to help their employees have the same experience that I described to provide almost Eric Topol like guidance service to help people find access to high quality care, which might be referring them into the community or to an academic medical center, but often is also us providing care delivery ourselves through on-demand primary care, urgent care, behavioral health. And now just last year we introduced a couple of our first specialty lines. And the idea, Eric, is that these companies buy this because they know their employees will love it and they do. It is often one of, if not the most highly rated benefits available. But also because in getting their employees better care faster, the employees come back to work, they feel more connected to the company, they're able to do better and safer and higher quality work. And they get more mileage out of their health benefits. And you have to remember that the costs of health benefits in this country are inflating even in this time of hyperinflation. They're inflating faster than anything else, and this is one of most companies, number one pain points for how they are going to control their overall budget. So this is a solution that both give them visibility to controlling cost and can deliver them an excellent patient experience that is not an offer that they've been able to get from the traditional managed care operators.Eric Topol (14:11):So I guess there's a kind of multidimensional approach that you're describing. For one, you can help find a doctor that's the right doctor for the right patient. And you're also actually providing medical services too, right?Owen Tripp (14:27):That's right.Eric Topol (14:30):Are these physicians who are employed by Included Health?Owen Tripp (14:34):They are, and we feel very strongly about that. We think that in our model, we want to train people, hire people in a specific way, prepare them for the kind of work that we do. And there's a lot we could spend time talking about there, but one of the key features of that is teamwork. We want people to work in a collaborative model where they understand that while they may be expert in one specific thing that is connected to a service line, they're working in a much broader team in support of the member, in support of that patient. And we talk about the patients being very first here, and you and I had a laugh on this in the past, so many hospitals will say we're patient first. So many managed care companies will say they're patient first, but it is actually hard the way that the system is designed to truly be patient first. At Included Health, we measure whether patients will come back to us, whether they tell their friends about us, whether they have high quality member satisfaction and are they living more healthy days. So everybody gets surveyed for patient reported outcomes, which is highly unusual as you know, to have both the clinical outcomes and the patient reported outcomes as well.Eric Topol (15:41):Is that all through virtual visits or are there physical visits as well?Owen Tripp (15:47):Today that is all through virtual visits. So we provide 24/7/365 access to urgent care, primary care, behavioral health, the start of the specialty clinic, which we launched last year. And then we provide support for patients who have questions about how these things are going to be billed, what other benefits they have access to. And where appropriate, we send them out to care. So obviously we can't provide all the exams virtually. We can't provide everything that a comprehensive physical would today, but as you and I know that is also changing rapidly. And so, we can do things to put sensors and other observational devices in people's homes to collect that data positively.Eric Topol (16:32):Now, how is that different than Teladoc and all these other telehealth based companies? I mean because trying to understand on the one hand you have a service that you can provide that can be extremely helpful and seems to be relatively unique. Whereas the other seems to be shared with other companies that started in this telehealth space.Owen Tripp (16:57):I think the easiest way to think about the difference here is how a traditional telemedicine company is paid and how we're paid because I think it'll give you some clue as to why we've designed it the way we've designed it. So the traditional telehealth model is you put a quarter in the jukebox, you listen to a song when the song's over, you got to get out and move on with the rest of your life. And quite literally what I mean is that you're going to see one doctor, one time, you will never see that same doctor again. You are not going to have a connected experience across your visits. I mean, you might have an underlying chart, but there's not going to be a continuity of care and follow up there as you would in an integrated setting. Now by comparison, and that's all derived from the fact that those telehealth companies are paid by the drink, they're paid by the visit.Owen Tripp (17:49):In our model, we are committing to a set of experience goals and a set of outcomes to the companies that you refer to that pay our bill. And so, the visits that our members enjoy are all connected. So if you have a primary care visit, that is connected to your behavioral health visit, which is great and is as it should be. If you have a primary care appointment where you identify the need for follow-up cardiology for example. That patient can be followed through that cardiology visit that we circle back, that we make sure that the patient is educated, that he or she has all their questions answered. That's because we know that if the patient actually isn't confident in what they heard and they don't follow through on the plan, then it's all for naught. It's not going to work. And it's a simple sort of observation, but it's how we get paid and why we think it's a really important way to think about medicine.Eric Topol (18:44):So these companies, and they're pretty big companies like Google and AT&T and as you said, JPMorgan and the list goes on and on. Any one of the employees can get this. Is that how it works?Owen Tripp (18:56):That's right, that's right. And even better, most of what I've described to you today is at a low or zero cost to them. So this is a very affordable, easy way to access care. Thinking about one of our very large airline clients the other day, we're often dealing with their flight crews and ramp agents at very strange hours in very strange places away from home, so that they don't have to wait to get access to care. And you can understand that at a basic humanitarian level why that's great, but you can also understand it from a safety perspective that if there is something that is impeding that person's ability to be functioning at work, that becomes an issue for the corporation itself.Eric Topol (19:39):Yeah, so it's interesting you call it included because most of us in the country are excluded. That is, they don't have any way to turn through to get help for a really good referral. Everything's out of network if they are covered and they're not one of the fortunate to be in these companies that you're providing the service for. So do you have any peers or are there any others that are going to come into this space to help a lot of these people that are in a tough situation where they don't really have anyone to turn to?Owen Tripp (20:21):Well, I hope so. Because like you, I've dedicated my career to trying to use information and use science and use in my own right to bring along the model. At Included Health, we talk about raising the standard of care for everybody, and what we mean by that is, we actually hope that this becomes a model that others can follow. The same way the Cleveland Clinic did, the same way the Mayo Clinic did. They brought a model into the world that others soon try to replicate, and that was a good thing. So we'd like to see more attempt to do this. The reality is we have not seen that because unfortunately the old system has a lot of incentives in place to function exactly the way that it is designed. The health system is going to maximize the number of patients that correspond to the highest paying procedures and tests, et cetera. The managed care company is going to try to process the highest number of claims, work the most efficient utilization management and prior authorization, but left out in the middle of all of that is the patient. And so, we really wanted to build that model with the patient at the center, and when I started this company now over a decade ago, that was just a dream that we could do that. Now serving over 10 million members, this feels like it's possible and it feels like a model others could follow.Eric Topol (21:50):Yeah, well that was what struck me is here you're reaching 10 million people. I'd never heard of it. I was like, wow. I thought I try to keep up with things. But now the other thing I wanted to get into you with is AI. Obviously, that has a lot of promise in many different ways. As you know, there are some 12 million diagnostic serious errors a year in the US. I mean you were one, I've been part of them. Most people have been roughed up one way or another. Then there's 800,000 Americans who have disability or die from these errors a year, according to Johns Hopkins relatively recent study. So one of the ways that AI could help is accuracy. But of course, there's many other ways it can help make the lives of both patients helping to integrate their data and physicians to go through a patient's records and set points of their labs and all sorts of other things. Where do you see AI fitting into the model that you've built?Owen Tripp (22:58):Well, I'll give you two that I'm really excited about, that I don't think I hear other people talking about. And again, I'm going to start with that patient, with that member and what he or she wants and needs. One and Eric, bear with me, this is going to sound very banal, but one is just making sense of these very complicated plan documents and explanations of benefits. I'm aware of how well-trained you are and how much you've written. I believe you are the most published in your field. I believe that is a fact. And yet if I showed you a plan description document and an explanation of benefit and I asked you, Eric, could you tell me how much it's going to cost to have an MRI at this facility? I don't think you would've any way of figuring that out. And that is something that people confront every single day in this country. And a lot of people are not like you and me, in that we could probably tolerate a big cost range for that MRI. For some people that might actually be the difference between whether they eat or not, or get their kids prescription or not.Owen Tripp (24:05):And so, we want to make the questions about what your benefits cover and how you understand what's available to you in your plan. We want to make that really easy and we want to make it so that you don't have to have a PhD in insurance language to be able to ask the properly formatted question. As you know, the foundation models are terrific at that problem. So that's one.Eric Topol (24:27):And that's a good one, that's very practical and very much needed. Yeah.Owen Tripp (24:32):The second one I'm really excited about, and I think this will also be near and dear to your heart, is AI has this ability to be sort of nonjudgmental in the best possible way. And so, if we have a patient on a plan to manage hypertension or to manage weight or to manage other elements of a healthy lifestyle. And here we're not talking about deep science, we're just talking about what we've known to work for a long period of time. AI as a coach to help follow through on those goals and passively take data on how you're progressing, but have behind it the world's greatest medical team to be able to jump in when things become more acute or more complex. That's an awesome tool that I think every person needs to be carrying around, so that if my care plan or if my goal is about sleeping better, if my goal is about getting pregnant, if my goal is about reducing my blood pressure, that I can do that in a way that I can have a conversation where I don't feel as a patient that I'm screwing up or letting somebody down, and I can be honest with that AI.Owen Tripp (25:39):So I'm really excited about the potential for the AI as an adjunct coach and care team manager to continue to proceed along with that member with medical support behind that when necessary.Eric Topol (25:55):Yeah, I mean there's a couple of things I'd say about that. Firstly, the fact that you're thinking it from the patient perspective where most working in AI is thinking it from the clinician perspective, so that's really important. The next is that we get notifications, and you need to not sit every hour or something like that from a ring or from a smartwatch or whatever. That isn't particularly intelligent, although it may be needed. The point is we don't get notifications like, what was your blood pressure? Or can you send a PDF of your heart rhythm or this sort of thing. Now the problem too is that people are generating lots of data just by wearing a smartwatch or a fitness band. You've got your activity, your sleep, your heart rate, and all sorts of things that are derivatives of that. No less, you could have other sensors like a glucose monitoring and on and on. No less your electronic health record, and there's no integration of any of this.Eric Topol (27:00):So this idea that we could have a really intelligent AI virtual coach for the patient, which as you said could have connects with a physician as needed, bringing in the data or bringing in some type of issue that the doctor needs to attend to, but it doesn't seem like anything is getting done. We have the AI capabilities, but nothing's getting done. It's frustrating because I wrote about this in 2019 in the Deep Medicine book, and it's just like some of the most sophisticated companies you would think Apple, for the ring Oura and so many others. They have the data, but they don't integrate anything, and they don't really set up notifications for patients. How are we going to get out of this rut?Owen Tripp (27:51):We are producing oil tankers of data around personal experience and not actually turning that into positive energy for what patients can do. But I do want to be optimistic on this point because I actually think, and I shared this with you when we last saw each other. Your thinking was ahead of the time, but foundational for people like me to say, we need to go actually make that real. And let me explain to you what I mean by making it real. We need to bring together the insight that you have an elevated heart rate or that your step count is down, or that your sleep schedule is off. We need to bring that together with the possibility of connecting with a medical professional, which these devices do not have the ability to do that today, and nor do those companies really want to get in that business. And also make that context of what you can afford as a patient.Owen Tripp (28:51):So we have data that's suggestive of an underlying issue. We have a medical team that's prepared to actually help you on that issue. And then we have financial security to know that whatever is identified actually will be paid for. Now, that's not a hard triangle conceptually, but no one of those companies is actually interested in all the points of the triangle, and you have to be because otherwise it's not going to work for the patient. If your business is in selling devices. Really all I'm thinking about is how do I sell devices and subscriptions. If my business is exclusively in providing care, that's really all I'm thinking about. If my business is in managing risk and writing insurance policies, that's really all I'm thinking about. You have to do all those three things in concert.Eric Topol (29:34):Yeah, I mean in many ways it goes back to what we were talking about earlier, which is we're in this phenomenal era of information to the fifth power. But here we are, we have a lot of data from multiple sources, and it doesn't get integrated. So for example, a person has a problem and they don't know what is the root cause of it. Let's say it's poor sleep, or it could be that they're having stress, which would be manifest through their heart rate or heart rate variability or all sorts of other metrics. And there's no intelligence provided for them to interpret their data because it's all siloed and we're just not really doing that for patients. I hope that'll happen. Hopefully, Included Health could be a lead in that. Maybe you can show the way. Anyway, this has been a fun conversation, Owen. It's rare that I've talked in Ground Truths with any person running a company, but I thought yours.Eric Topol (30:36):Firstly, I didn't know anything about it and it’s big. And secondly, that it's a kind of a unique model that really I'm hoping that others will get involved in and that someday we'll all be included. Maybe not with Included Health, but with better healthcare in this country, which is certainly not the norm, not the routine. And also, as you aptly pointed out at terrible costs with all sorts of waste, unnecessary tests and that sort of thing. So thanks for what you're doing and I'll be following your future efforts and hopefully we can keep making some strides.Owen Tripp (31:15):We will. And I wanted to say thanks for the conversation too and for your thinking on these topics. And look, I want to leave you just with a quick dose of optimism, and you and I both know this. The American system at its best is an extraordinary system, unrivaled in the world, in my opinion. But we do have to have more people included. All the services need to be included in one place. When we get there, we're going to really see what's possible here.Eric Topol (31:40):I do want to agree with you that if you can get to the right doctor and if you can afford it, that is ideally covered by your insurance. It is a phenomenal system, but getting there, that's the hard part. And every day people are confronted. I'm sure, thousands and thousands with serious condition either to get the diagnosis or the treatment, and they have a really rough time. So anyway, so thank you and I really appreciate your taking the time to meet with me today.****************************************************************Thanks for listening, watching, reading and subscribing to Ground Truths.An update on Super Agers:It is ranked #5 on the New York Times bestseller list (on the list for 4th time)https://www.nytimes.com/books/best-sellers/advice-how-to-and-miscellaneous/New podcastsPBS Walter Isaacson, Amanpour&Co Factually, With Adam ConoverPeter Lee, Microsoft Researchhttps://x.com/MSFTResearch/status/1943460270824714414If you found this interesting PLEASE share it!That makes the work involved in putting these together especially worthwhile.Thanks to Scripps Research, and my producer, Jessica Nguyen, and Sinjun Balabanoff for video/audio support.All content on Ground Truths—its newsletters, analyses, and podcasts, are free, open-access.Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don't hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. Get full access to Ground Truths at erictopol.substack.com/subscribe | 32m 27s | ||||||
| 7/8/25 |  Priscilla Chan & Jennifer Doudna: New Center for Pediatric CRISPR Cures | Eric Topol (00:05):Hello, it's Eric Topol from Ground Truths, and I've got some really exciting stuff to talk to you about today. And it's about the announcement for a new Center for pediatric CRISPR Cures. And I'm delight to introduce doctors Jennifer Doudna and Priscilla Chan. And so, first let me say this is amazing to see this thing going forward. It's an outgrowth of a New England Journal paper and monumental report on CRISPR in May. [See the below post for more context]Let me introduce first, Dr. Doudna. Jennifer is the Li Ka Shing Chancellor's Chair and a Professor in the departments of chemistry and of molecular and cell biology at the University of California Berkeley. She's also the subject of this book, one of my favorite books of all time, the Code Breaker. And as you know, the 2020 Nobel Prize laureate for her work in CRISPR-Cas9 genome editing, and she founded the Innovative Genomics Institute (IGI) back 10 years ago. So Jennifer, welcome.Jennifer Doudna (01:08):Thank you, Eric. Great to be here.Eric Topol (01:10):And now Dr. Priscilla Chan, who is the co-founder of the Chan Zuckerberg Initiative (CZI) that also was started back in 2015. So here we are, a decade later, these two leaders. She is a pediatrician having trained at UCSF and is committed to the initiative which has as its mission statement, “to make it possible to cure, prevent, and manage all diseases in this century.” So today we're going to talk about a step closer to that. Welcome, Priscilla.Priscilla Chan (01:44):Thank you. Thanks for having me.Eric Topol (01:46):Alright, so I thought we'd start off by, how did you two get together? Have you known each other for over this past decade since you both got all your things going?Jennifer Doudna (01:56):Yes, we have. We've known each other for a while. And of course, I've admired the progress at the CZI on fundamental science. I was an advisor very early on and I think actually that's how we got to know each other. Right, Priscilla?Priscilla Chan (02:11):Yeah, that's right. We got to know each other then. And we've been crisscrossing paths. And I personally remember the day you won the Nobel Prize. It was in the heart of the pandemic and a lot of celebrations were happening over Zoom. And I grabbed my then 5-year-old and got onto the UCSF celebration and I was like, look, this is happening. And it was really cool for me and for my daughter.Eric Topol (02:46):Well, it's pretty remarkable convergence leading up to today's announcement, but I know Priscilla, that you've been active in this rare disease space, you've had at CZI a Rare As One Project. Maybe you could tell us a bit about that.Priscilla Chan (03:01):Yeah, so at CZI, we work on basic science research, and I think that often surprises people because they know that I'm a pediatrician. And so, they often think, oh, you must work in healthcare or healthcare delivery. And we've actually chosen very intentionally to work in basic science research. In part because my training as a pediatrician at UCSF. As you both know, UCSF is a tertiary coronary care center where we see very unusual and rare cases of pediatric presentations. And it was there where I learned how little we knew about rare diseases and diseases in general and how powerful patients were. And that research was the pipeline for hope and for new discoveries for these families that often otherwise don't have very much access to treatments or cures. They have a PDF that maybe describes what their child has. And so, I decided to invest in basic science through CZI, but always saw the power of bringing rare disease patient cohorts. One, because if you've ever met a parent of a child with rare disease, they are a force to be reckoned with. Two, they can make research so much better due to their insights as patients and patient advocates. And I think they close the distance between basic science and impact in patients. And so, we've been working on that since 2019 and has been a passion of ours.Eric Topol (04:40):Wow, that's great. Now Jennifer, this IGI that you founded a decade ago, it's doing all kinds of things that are even well beyond rare diseases. We recently spoke, I know on Ground Truths about things as diverse as editing the gut microbiome in asthma and potentially someday Alzheimer’s. But here you were very much involved at IGI with the baby KJ Muldoon. Maybe you could take us through this because this is such an extraordinary advance in the whole CRISPR Cures story.Jennifer Doudna (05:18):Yes, Eric. It's a very exciting story and we're very, very proud of the teamwork that went into making it possible to cure baby KJ of his very rare disease. And in brief, the story began back in August of last year when he was born with a metabolic disorder that prevented him from digesting protein, it's called a urea cycle disorder and rare, but extremely severe. And to the point where he was in the ICU and facing a very, very difficult prognosis. And so, fortunately his clinical team at Children's Hospital of Philadelphia (CHOP) reached out to Fyodor Urnov, who is the Director of Translational Medicine at the IGI here in the Bay Area. They teamed up and realized that they could quickly diagnose that child because we had an IRB approved here at the IGI that allowed us to collect patient samples and do diagnosis. So that was done.Jennifer Doudna (06:26):We created an off-the-shelf CRISPR therapy that would be targeted to the exact mutation that caused that young boy's disease. And then we worked with the FDA in Washington to make sure that we could very safely proceed with testing of that therapy initially in the lab and then ultimately in two different animal models. And then we opened a clinical trial that allowed that boy to be enrolled with, of course his parents' approval and for him to be dosed and the result was spectacular. And in fact, he was released from the hospital recently as a happy, healthy child, gaining lots of weight and looking very chunky. So it's really exciting.Eric Topol (07:16):It's so amazing. I don't think people necessarily grasp this. This timeline [see above] that we'll post with this is just mind boggling how you could, as you said Jennifer, in about six months to go from the birth and sequencing through cell specific cultures with the genome mutations through multiple experimental models with non-human primates even, looking at off-target effects, through the multiple FDA reviews and then dosing, cumulatively three dosing to save this baby's life. It really just amazing. Now that is a template. And before we go to this new Center, I just wanted to also mention not just the timeline of compression, which is unimaginable and the partnership that you've had at IGI with I guess Danaher to help manufacture, which is just another part of the story. But also the fact that you're not just even with CRISPR 1.0 as being used in approvals previously for sickle cell and β-thalassemia, but now we're talking about base editing in vivo in the body using mRNA delivery. So maybe you could comment on that, Jennifer.Jennifer Doudna (08:38):Yeah, very good point. So yeah, we used a version of CRISPR that was created by David Liu at the Broad Institute and published and available. And so, it was possible to create that, again, targeted to the exact mutation that caused baby KJ’s disease. And fortunately, there was also an off-the-shelf way to deliver it because we had access to lipid nanoparticles that were developed for other purposes including vaccinations. And the type of disease that KJ suffered from is one that is treatable by editing cells in the liver, which is where the lipid nanoparticle naturally goes. So there were definitely some serendipity here, but it was amazing how all of these pieces were available. We just had to pull them together to create this therapy.Eric Topol (09:30):Yeah, no, it is amazing. So that I think is a great substrate for starting a new Center. And so, maybe back to you Priscilla, as to what your vision was when working with Jennifer and IGI to go through with this.Priscilla Chan (09:45):I think the thing that's incredibly exciting, you mentioned that at CZI our mission is to cure, prevent, and manage all disease. And when we talked about this 10 years ago, it felt like this far off idea, but every day it seems closer and closer. And I think the part that's super exciting about this is the direct connection between the basic science that's happening in CRISPR and the molecular and down to the nucleotide understanding of these mutations and the ability to correct them. And I think many of us, our imaginations have included this possibility, but it's very exciting that it has happened with baby KJ and CHOP. And we need to be able to do the work to understand how we can treat more patients this way, how to understand the obstacles, unblock them, streamline the process, bring down the cost, so that we better understand this pathway for treatment, as well as to increasingly democratize access to this type of platform. And so, our hope is to be able to do that. Take the work and inspiration that IGI and the team at CHOP have done and continue to push forward and to look at more cases, look at more organ systems. We're going to be looking in addition to the liver, at the bone marrow and the immune system.Priscilla Chan (11:17):And to be able to really work through more of the steps so that we can bring this to more families and patients.Eric Topol (11:30):Yeah, well it's pretty remarkable because here you have incurable ultra-rare diseases. If you can help these babies, just think of what this could do in a much broader context. I mean there a lot of common diseases have their roots with some of these very rare ones. So how do you see going forward, Jennifer, as to where you UC Berkeley, Gladstone, UCSF. I'm envious of you all up there in Northern California I have to say, will pull this off. How will you get the first similar case to KJ Muldoon going forward?Jennifer Doudna (12:13):Right. Well, IGI is a joint institute, as you probably know, Eric. So we were founded 10 years ago as a joint institute between UC Berkeley and UCSF. And now we have a third campus partner, UC Davis and we have the Gladstone Institute. So we've got an extraordinary group of clinicians and researchers that are coming together for this project and the Center to make it a success. We are building a clinical team at UCSF. We have several extraordinary leaders including Jennifer Puck and Chris Dvorak, and they are both going to be involved in identifying patients that could be enrolled in this program based on their diagnosis. And we will have a clinical advisory group that will help with that as well. So we'll be vetting patients probably right after we announce this, we're going to be looking to start enrolling people who might need this type of help.Eric Topol (13:18):Do you think it's possible to go any faster right now than the six months that it took for KJ?Jennifer Doudna (13:26):I think it could be. And here's the reason. There's a very interesting possibility that because of the type of technology that we're talking about with CRISPR, which fundamentally, and you and I have talked about this previously on your other podcast. But we've talked about the fact that it's a programmable technology and that means that we can change one aspect of it, one piece of it, which is a piece of a molecule called RNA that's able to direct CRISPR to the right sequence where we want to do editing and not change anything else about it. The protein, the CRISPR protein stays the same, the delivery vehicle stays the same, everything else stays the same. And so, we're working right now with FDA to get a platform designation for CRISPR that might allow streamlining of the testing process in some cases. So it'll obviously come down to the details of the disease, but we're hopeful that in the end it will be possible. And Priscilla and I have talked about this too, that as AI continues to advance and we get more and more information about rare diseases, we'll be able to predict accurately the effects of editing. And so, in some cases in the future it may be possible to streamline the testing process even further safely.Eric Topol (14:51):And I also would note, as you both know, well this administration is really keen on genome editing and they've had a joint announcement regarding their support. And in my discussions with the FDA commissioner, this is something they are very excited about. So the timing of the new Center for pediatric CRISPR Cures is aligned with the current administration, which is good to see. It's not always the case. Now going back, Priscilla, to your point that not just for the liver because delivery has been an issue of course, and we're going to try to get after a lot of these really rare diseases, it's going to go beyond there. So this is also an exciting new dimension of the Center, as you said, to go after the bone marrow for hematopoietic cells, perhaps other organs as well.Priscilla Chan (15:42):I mean what the expertise and feasibility, the immune system is going to be the next target. Jennifer Puck has been a pioneer in this work. She's the one who designed the newborn screen that will be the tool that picks up these patients as they are born. And I think the thing that's tremendous is the immune system, first of all is active in many, many diseases, not just these cases of children born with partial or absence of immune systems. And the course right now that these babies are left with is complete isolation and then a very long and arduous course of a bone marrow transplant with high morbidity and mortality. And even if after the transplant you have complications like graft versus host and immunosuppression. And so, the idea of being able to very specifically and with less the conditioning and morbidity and mortality of the treatment, being able to address this is incredible. And the implications for other diseases like blood cancers or other hematopoietic diseases, that's incredible. And that actually has an incredibly broad base of patients that can benefit from the learnings from these babies with severe combined immunodeficiencies.Eric Topol (17:10):Yeah, I think that goes back to a point earlier maybe to amplify in that previous CRISPR generation, it required outside the body work and it was extremely laborious and time consuming and obviously added much more to the expense because of hospitalization time. This is different. This is basically doing this inside the affected patient's body. And that is one of the biggest reasons why this is a big step forward and why we're so fortunate that your Center is moving forward. Maybe before we wrap up, you might want to comment, Jennifer on how you were able to bring in to build this platform, the manufacturing arm of it, because that seems to be yet another dimension that's helpful.Jennifer Doudna (18:01):Indeed, yes. And we were again fortunate with timing because you mentioned briefly that the IGI had set up a program with the Danaher Corporation back in January of last year. We call it our Beacon project. And it's focused on rare disease. And it's a really interesting kind of a unique partnership because Danaher is a manufacturing conglomerate. So they have companies that make molecules, they make proteins, they make RNA molecules, they make delivery molecules. And so, they were excited to be involved with us because they want to be a provider of these types of therapies in the future. And they can see the future of CRISPR is very exciting. It's expanding, growing area. And so, that agreement was in place already when the baby KJ case came to our attention. And so, what we're hoping to do with Danaher is again, work with them and their scientists to continue to ask, how can we reduce the cost of these therapies by reducing the cost of the molecules that are necessary, how to make them efficiently. We already, it's very interesting, Fyodor Urnov has toured their plant in North Dakota recently, and he found in talking to their engineers, there are a number of things that we can already see will be possible to do that are going to make the process of manufacturing these molecules faster and cheaper by a lot.Eric Topol (19:28):Wow.Jennifer Doudna (19:28):So it's a win-win for everybody. And so, we're really excited to do that in the context of this new Center.Eric Topol (19:36):Oh, that's phenomenal because some of these disorders you don't have that much time to work with before they could be brain or organ or vital tissue damage. So that's great to hear that. What you built here is the significance of it can't be under emphasized, I'll say because we have this May report of baby KJ, which could have been a one-off and it could have been years before we saw another cure of an ultra-rare disorder. And what you're doing here is insurance against that. You're going to have many more cracks at this. And I think this is the excitement about having a new dedicated Center. So just in closing, maybe some remarks from you Priscilla.Priscilla Chan (20:24):I just want to emphasize one point that's really exciting as we talk about these ultra-rare cases that they're often like one in a million. All these learnings actually help maximize the impact of lots of research across the sector that impacts actually everyone's health. And so, our learnings here from these patients that have very significant presentations that really can stand to benefit from any treatment is hopefully paving the way for many, many more of us to be able to live healthier, higher quality lives through basic science.Eric Topol (21:13):And over to you, Jennifer.Jennifer Doudna (21:15):Couldn't agree more. It's a really interesting moment. I think what we hope we are, is we're at sort of an inflection point where, as I mentioned earlier, all the pieces are in place to do this kind of therapeutic and we just need a team that will focus on doing it and pulling it together. And also learning from that process so that as Priscilla just said, we are ultimately able to use the same strategy for other diseases and potentially for diseases that affect lots of people. So it's exciting.Eric Topol (21:46):For sure. Now, if I could just sum up, this is now a decade past the origination of your work of CRISPR and how already at the first decade culminated in sickle cell disease treatment and β-thalassemia. Now we're into the second decade of CRISPR. And look what we've seen, something that was unimaginable until it actually happened and was reported just a little over a month ago. Now going back to Priscilla's point, we're talking about thousands of different rare Mendelian genomic disorders, thousands of them. And if you add them all up of rare diseases, we're talking about hundreds of millions of people affected around the world. So this is a foray into something much bigger, no less the fact that some of these rare mutations are shared by common diseases and approaches. So this really big stuff, congratulations to both of you and your organizations, the Innovative Genomics Institute and the Chan Zuckerberg Initiative for taking this on. We'll be following it with very deep interest, thank you.****************************************************Thanks for listening, reading and subscribing to Ground Truths.If you found this interesting PLEASE share it!That makes the work involved in putting these together especially worthwhile.Thanks to Scripps Research, and my producer, Jessica Nguyen, and Sinjun Balabanoff for video/audio support.All content on Ground Truths—its newsletters, analyses, and podcasts, are free, open-access.Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don't hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. Get full access to Ground Truths at erictopol.substack.com/subscribe | 23m 08s | ||||||
Showing 25 of 89
Sponsor Intelligence
Sign in to see which brands sponsor this podcast, their ad offers, and promo codes.
Similar Audience Demographics
Podcasts that attract a similar listener profile






Chart Positions
42 placements across 39 markets.
Chart Positions
42 placements across 39 markets.