Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Most discussed topics
Brands & references
Total monthly reach
Estimated from 1 chart position in 1 market.
By chart position
- 🇮🇸IS · Mental Health#174500 to 3K
- Per-Episode Audience
Est. listeners per new episode within ~30 days
250 to 1.5K🎙 ~2x weekly·122 episodes·Last published 1mo ago - Monthly Reach
Unique listeners across all episodes (30 days)
500 to 3K🇮🇸100% - Active Followers
Loyal subscribers who consistently listen
200 to 1.2K
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
From 10 epsHosts
Recent guests
No guests detected in recent episodes.
Recent episodes
Why We Can't Separate Our Childhood From Our Physiology (& Biochemistry)
May 5, 2026
23m 30s
How Nutrients Impact Neurotransmitters & Walsh Data
Apr 19, 2026
14m 22s
Children, Teens & Technology: Research & Resources for Parents
Mar 27, 2026
9m 45s
Stop Chasing "Anti-Aging." Lower Oxidative Stress Instead
Mar 7, 2026
7m 51s
Stop Saying “Underage” & Other Words That Blur the Lines
Feb 19, 2026
16m 17s
Social Links & Contact
Official channels & resources
Official Website
Login
RSS Feed
Login
| Date | Episode | Topics | Guests | Brands | Places | Keywords | Sponsor | Length | |
|---|---|---|---|---|---|---|---|---|---|
| 5/5/26 |  Why We Can't Separate Our Childhood From Our Physiology (& Biochemistry)✨ | Adverse Childhood ExperiencesPhysiology+3 | — | Holistic Psychiatry PodcastPositive Adaptive Childhood Experiences Study+1 | — | ACEsPCEs+3 | — | 23m 30s | |
| 4/19/26 |  How Nutrients Impact Neurotransmitters & Walsh Data✨ | nutrientsneurotransmitters+4 | — | Walsh Research Institute | — | nutrient impactneurotransmitter function+6 | — | 14m 22s | |
| 3/27/26 |  Children, Teens & Technology: Research & Resources for Parents✨ | impact of screen mediamental health+4 | — | MetaYouTube+2 | — | screen timemental health+6 | — | 9m 45s | |
| 3/7/26 |  Stop Chasing "Anti-Aging." Lower Oxidative Stress Instead✨ | oxidative stressaging+5 | — | — | — | oxidative stressanti-aging+5 | — | 7m 51s | |
| 2/19/26 |  Stop Saying “Underage” & Other Words That Blur the Lines✨ | language and abusenormalization of abuse+3 | — | — | — | abuselanguage+5 | — | 16m 17s | |
| 1/31/26 |  The Physiologic Roots of Panic - A Holistic Approach | In this episode, I discuss panic attacks and underlying vulnerabilities that can increase the sensitivity of our alarm system. * What is a panic attack and what does it feel like? * What neurotransmitters are involved?* What is panic disorder?* What nutritional, genetic, and hormonal factors can be at play?* What types of inflammation and toxicity can lead to panic attacks?* How do the immune, limbic and autonomic nervous system contribute?* How does insecure attachment, trauma and stress interact with these other vulnerabilities?Takeaways* Panic attacks occur when the brain’s alarm system is overly sensitive.* Physical symptoms of panic attacks can be debilitating and terrifying.* Underlying physiological factors contribute to vulnerability to panic attacks.* Neurotransmitters like norepinephrine and GABA play crucial roles in panic disorders.* Hormonal imbalances, especially in women, can increase the likelihood of panic attacks.* Mast cells are involved in the immune response and can trigger panic symptoms.* Biotoxins, such as mold toxins, can contribute to mast cell activation, limbic system dysfunction and autonomic nervous system dysfunction* Limbic system dysfunction can lead to heightened anxiety and panic.* The autonomic nervous system regulates our fight or flight response.* Emotional stressors and trauma can contribute to panic attacks, but appear to be aligning with other physiologic vulnerabilitiesChapters00:00 Understanding Panic Attacks03:07 Physiological Factors Behind Panic Attacks06:00 Neurotransmitters, Nutrient Levels and Panic Disorder08:52 The Role of Genetic Variants & Hormones in Panic Attacks12:07 Inflammation and Panic Attacks14:53 Mast Cells - The Bridge Between the Immune & Central Nervous Systems18:06 Biotoxins and Their Impact on Panic21:00 Limbic System Dysfunction and Panic24:11 The Autonomic Nervous System’s Role26:45 Emotional Stressors and Panic AttacksAs always, I welcome any comments and questions. Your interests and what you care about helps guide the information I share. Also, its really nice for me to be in conversation and learning from you.Until next time,CourtneyTo learn more about my discovery calls, non-patient consultations, or mentoring, please visit my website at:CourtneySnyderMD.comMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for either yourself or others, including but not limited to patients that you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 29m 20s | ||||||
| 11/11/25 |  Mold Toxicity: A Common Cause of Brain Symptoms | In this episode, I discuss:* Mold related illness, with a focus on mold toxicity and mold colonization* The wide range of brain symptoms (and other symptoms associated with mold toxicity* How we can become exposed to toxic mold even when we don’t see mold growth* Why not everyone with the same exposure doesn’t become toxic* How mold toxicity is diagnosed* How we can test our environment for mold* The four core aspects of treatment: removing exposure, using binders to eliminate toxins, addressing fungal colonization if present, and adjusting diet to avoid feeding mold and candida, which often is present in those with mold toxicity* The importance of addressing mast cell activation, limbic system retraining and vagal nerve interventions for those who are highly sensitive to treatment interventions* Practical steps such as air purification, humidity controlIn the next episode, I will be reviewing research exploring the connection between mold and brain related conditions — and address the question, “Does mold enter the brain, in those who are not obviously immunocompromised?”Rarely does mold toxicity occur in isolation. It will often contribute to other root causes, such as mast cell activation, electromagnetic hypersensitivity, multiple chemical sensitivity, increased pyrroles, worsening of copper zinc imbalances, decreased methylation, and an increased risk of other microbial activations or autoimmunity.As always, I welcome any comments and questions, as these help guide the information that I share.Until next time,CourtneyTo learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for either yourself or others, including but not limited to patients that you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 15m 53s | ||||||
| 10/30/25 |  Compulsive Caregiving - A Common But Less Obvious Attachment Pattern | In this episode, I explore compulsive caregiving from an attachment perspective. This is a more subtle form of insecure attachment that nonetheless affects one’s ability to thrive and enjoy healthy relationships. Related terms include over-functioning, codependency, and Nice Guy / Good Girl Syndrome.This is the fourth of a four-part series on how our experiences with caregivers in the first three years of life can impact our emotional regulation, beliefs about ourselves, and adult relationships.Here I discuss:* How early attachment experiences shape compulsive caregiving and the “parentified child” dynamic* How over-functioning, people-pleasing, and codependency share a common root in early life and are an attempt to manage attachment anxiety* How physiologic differences, especially of those who are highly sensitive (HSP/Highly Sensitive Person), may make them more vulnerable* The similarities to other addictive and compulsive behaviors* Where this attachment style would fall if placed on the attachment spectrum* The beliefs, emotional states, behaviors, and communication styles that can be present when someone struggles with compulsive caregiving.* The physical and psychological toll of the often-present chronic stress and emotional repression* Tools and interventions that can help one move towards healing and thriving* Specific resources that support awareness and recovery, including The Drama of the Gifted Child, Adult Children of Emotionally Immature Parents, and Codependent No MoreAs always, I welcome any comments and questions, as these help guide the information that I share.Until next time,CourtneyTo learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comLinks to related content:Compulsive Caregiving, Over-functioning, Codependency & Nice Guy/Good Girl SyndromeMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for either yourself or others, including but not limited to patients that you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 30m 22s | ||||||
| 10/20/25 |  The Cause of Bipolar Disorder - Recent Discovery by Dr. William Walsh | I am happy to share a recent conversation I had with Dr. William Walsh about his new book, “The Essence of Bipolar Disorder,” where he lays out his discovery into the cause of Bipolar Disorder, a condition with fluctuating high and low mood states that has baffled researchers and psychiatrists.Dr. Walsh, the president of the non-profit Walsh Research Institute, is an internationally recognized expert in the field of nutritional medicine. Dr. Walsh’s work in nutrient-based psychiatry began while collaborating with the renowned Carl C. Pfeiffer, MD, PhD (a pioneer in the field of nutritional psychiatry) to develop individualized nutrient protocols, originally focusing on violent and criminal behavior before expanding to ADHD, depression, anxiety, bipolar disorder, autism and schizophrenia. Dr. Walsh went on to study more than 30,000 patients with mental disorders, acquiring an unparalleled database of more than 3 million chemical assays during his clinical and research work. From this database, Dr. Walsh discovered the biotypes of depression, ADHD and Schizophrenia.Dr. Walsh has conducted chemical analysis of more than 25 serial killers. He has assisted medical examiners, Scotland Yard, and the FBI. He has designed nutritional programs for Olympic and professional athletes.In this episode, we discuss:* Bipolar Disorder, how it differs from other psychiatric conditions and why it has been so challenging for psychiatric researchers to understand.* The strong inheritance of Bipolar Disorder (despite a single gene never having been identified).* Dr. Walsh’s journey uncovering the cause of Bipolar Disorder, which started with studying the related neuroscience research, followed by a review of the emerging genetic research, specifically, the GWAS (Gene-Wide Association Study), which identified many genes related to bipolar disorder, to a focus on the ion channel genes, DNA repair genes and finally Bipolar Disorder as a “channelopathy.”* The alignment of genetic vulnerabilities involving ion channel genes and DNA repair genes and oxidative assault.* How the weakness of DNA damage genes can contribute to other health issues, accelerate aging, and lower life expectancy.* How weak ion channel genes can also contribute to high oxidative stress.* Bipolar Disorder as a “channelopathy”, and the explanation for switching from euthymia (normal mood) to mania to depression and back to euthymia (from a neurotransmission standpoint)* How this information impacts treatment and prevention.Related Content:Wash Research InstituteLunch with Dr. William Walsh - His Story, Discoveries & the Future of Nutrient-Based PsychiatryBreakthrough Theory of Bipolar DisorderAs always, I welcome any comments and questions, as these help guide the information that I share.Until next time,CourtneyTo learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for either yourself or others, including but not limited to patients that you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 1h 10m 37s | ||||||
| 10/7/25 |  Anxious-Preoccupied Attachment Style | In this episode, I discuss the anxious (ambivalent–preoccupied) attachment style — a pattern marked by intensity, dependence, and a longing for reassurance.I address how this attachment pattern develops, how it can appear in adulthood, and what kinds of therapeutic and holistic supports can help someone move toward a more secure attachment style. Specifically, I discuss:* How inconsistency in early caregiving (and even threats or experiences of abandonment) can lead to an anxious attachment style and problems with emotional regulation.* The key differences between anxious and avoidant attachment patterns* What the infant-toddler attachment research revealed about early caregiving and attachment dynamics* How anxious attachment can manifest as overwhelm, and fear of abandonment in adult relationships* Links between attachment and biochemical factors such as inflammation, methylation, high copper, high pyrroles, mast cell activation, and even biotoxin illness such as mold toxicity.* Psychotherapy approaches that promote regulation and security — including learning about healthy boundaries* The importance of structure, daily routines, and developing a reliable “inner parent”* Mind–body strategies such as guided meditation, goal-focused journaling, and creative learning* How addressing both emotional and biochemical roots can support long-term healing and resilienceWith awareness, compassion, education and support, we can rewire our nervous system toward greater calm, clarity, and self-trust.As always, I welcome your thoughts and questions.Until next time,CourtneyTo learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for either yourself or others, including but not limited to patients that you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 26m 59s | ||||||
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 9/11/25 |  Dismissive-Avoidant Attachment Style | What do the TV and film characters Don Draper (Mad Men), James Bond, Miranda Priestly (The Devil Wears Prada), and Rick Blaine (Casablanca) have in common? Each is a fairly good illustration of the Avoidant-Dismissive Attachment Style portrayed in film.In the last episode, I discussed how our experiences with caregivers during our first three years of life may continue to impact our ability to regulate emotions and form beliefs about ourselves and others. More deeply, I address how attachment shapes our neurophysiology - specifically our right and left hemisphere differentiation, our limbic system (“lizard brain”) and our autonomic nervous system.In this episode, I will focus more closely on one end of the attachment spectrum - the avoidant-dismissive attachment style. I’ll discuss:* How, in the early research, attachment was measured in toddlers and adults* How avoidant-dismissive attachment appears to develop* What it looks like in relationships* Personality Disorders that, if present, align with this type of attachment style* Similarities with undermethylation and how avoidant-dismissive attachment style may relate to undermethylation* The role of psychotherapy, group work, and supportive relationships in healing* Other tools, practices, and choices that can support healing.* How awareness of these patterns can transform not only personal well-being but also parenting and family dynamics across generationsOne theme I return to often is that growth is always possible. While avoidant attachment may develop early in life, it does not define a person forever. With curiosity, growing compassion, and the willingness to practice new ways of relating to ourselves and to others, we can expand our capacity for connection and begin to feel more whole.In the next episode, I look forward to discussing the other end of the attachment spectrum - the Anxious-Ambivalent (Preoccupied) Attachment Style.As always, I welcome any comments and questions, as these help guide the information that I share.Until next time,CourtneyTo learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comLinks to related content:Methylation & Brain HealthUndermethylation Myths, MTHFR & The Great Folate DebateMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for either yourself or others, including but not limited to patients that you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 29m 22s | ||||||
| 2/11/25 |  OCD & Nutrient Based Therapies | OCD, or Obsessive Compulsive Disorder, is a debilitating condition that involves intrusive thoughts and time-consuming, repetitive behaviors. It impacts 80 million worldwide, 2-4% of the US population or 1 in 100 people here in the US.It can be difficult to overstate the suffering caused by OCD, not only for those with this condition but also for their family members. In addition to the distress caused by the obsessional thoughts and compulsions, there can be shame and loss - loss of more meaningful, purposeful, or pleasant thoughts and behaviors. and loss of time connecting with others or engaging in purposeful or enjoyable activities.Other conditions associated with obsessive-compulsive disorder include:* Body dysmorphic disorder* Skin picking* Trichotillomania (hair pulling)* Hoarding* Hypochondria* Olfactory reference syndrome (an irrational feeling or belief that one emits a foul smell and often attempts to remove the odor).It´s not unusual for someone with OCD to have other conditions, such as:* Other forms of anxiety* Depression* ADHD* Autism spectrum disorder* Eating disorders* TourettesResearch suggests that having OCD raises one´s vulnerability to developing dementia. Many other brain conditions, however, also appear to increase this vulnerability similarly.Treatment ChallengesOCD is particularly challenging to treat. Of those with OCD, 60% do not respond to typical therapies (often medication in combination with psychotherapy involving gradual exposure to that which is being avoided). Typical medications include:* SSRI´s (Selective Serotonin Reuptake Inhibitors) -e.g., sertraline, fluoxetine, fluvoxamine, citalopram, paroxetine* Tricyclic antidepressant - clomipramine* SNRI - (Serotonin and Norepinephrine Reuptake Inhibitor) - venlafaxine* Atypical antipsychotic medications are sometimes addedMedication is combined with CBT (Cognitive Behavioral Therapy), which involves exposure and response prevention, or CBT is used alone.As you can see, most medication approaches aim to increase serotonin activity. Serotonin, however, is just one of the neurotransmitters involved. What has become increasingly clear from the research is that OCD involves abnormal activity at the NMDA receptor - a glutamate receptor.NMDA & GlutamateThe NMDA receptor is found throughout the brain. Glutamate, the primary excitatory neurotransmitter in the central nervous system, binds to the NMDA receptor. NMDA and glutamate are involved in synaptic plasticity (creating neuronal connections), learning, memory, and motor function.The synapse is the space between communicating neurons. Presynaptic neurons release glutamate, which binds to the NMDA receptor on postsynaptic neurons. This results in a cascade of signaling events that lead to “neuronal excitation.” The problem arises when this receptor has too much (or too little) activity. In the case of OCD, there is too much activity.Implications* Dysregulation at the NMDA receptor appears to play a role in OCD, depression, PTSD, schizophrenia, bipolar disorder, and substance use disorders.* Weak memory extinction can result from high activity at the NMDA receptor. While memory is a good thing, we can have problems with too much memory - or rather, problems putting our memories aside. This can look like thoughts getting stuck, for example:* Intrusive thoughts in OCD* Flashbacks in PTSD* Delusions in psychotic disorders* Cravings in addiction.* Neurodegenerative disorders, such as Alzheimer’s, Parkinson’s, and ALS, have also been linked to NMDA receptor malfunction.Methylation & NMDAThose who are undermethylated, especially those with OCD or addictions, have high activity at the NMDA receptor. To remind you, undermethylation is a biochemical process with many functions, including the breakdown of histamine, support of detoxification, and support of serotonin activity. When someone is undermethylated, they can tend to have allergies (from high histamine), be perfectionistic, competitive, strong-willed, have obsessive-compulsive tendencies, be ritualistic, have dietary inflexibility, and have high accomplishment or have family members with high accomplishment. Undermethylation can contribute to the low serotonin activity seen in OCD. Simply addressing undermethylation, like merely addressing serotonin, will only bring partial benefit. To address undermethylation, those of us trained by the Walsh Research Institute, use SAMe and/or methionine, B12, B6, magnesium, and antioxidants. We address this before starting methylation treatment for those with high homocysteine. But how can we also decrease activity at the NMDA receptor?Blocking NMDA & Normalizing Glutamate ActivityEsketamine or Ketamine, which has been getting much attention in recent years, can impact the brain in various ways; however, its primary mechanism is as an NMDA blocker or antagonist. For some, it can serve as a rapid-acting and highly effective antidepressant. It can also decrease OCD symptoms. Other NMDA-blocking drugs include memantine and dextromethorphan (combined with bupropion). Lamotrigine can decrease glutamate release and has been used as an adjunct medication for OCD.Nutrients, however, play an important role in the NMDA receptor. NAC or N-acetyl cysteine is a precursor to glutathione and, thus, an antioxidant. It is also anti-inflammatory and a binder for a particular toxin made by candida and mold. But, it is also a potent NMDA antagonist (decreases activity at NMDA) and has been shown to reduce obsessions and compulsions of OCD. It has also been studied in alcoholism, opiate addiction, cocaine abuse, gambling disorder, shopping disorder, cigarette addiction, and trichotillomania. It has been used by itself and as an adjunct to medication therapy. NAC has become part of the Walsh undermethylation nutrient protocols for those with OCD and/or addiction.Zinc also plays an important role in regulating functioning at the NMDA receptor. The Walsh Research Institute found that 90% of those with brain symptoms had relatively low zinc. Dosing of zinc is determined after testing plasma zinc levels using a narrow range (the Walsh/Pheiffer range differs from typical lab ranges). Zinc is checked in conjunction with copper. Zinc has been found to improve treatment response in those with OCD treated with SSRIs. Zinc can be depleted because of very high oxidative stress and/or high pyrroles, which also cause low B6. Because B6 is needed to make serotonin, pyrroles are also important to address if elevated.Inositol is a nutrient involved in the serotonin and glutamate signaling systems. It, too, is beneficial for OCD symptoms; however, it can require very high doses.The challenge of research, as you can see, is that these approaches are all looked at in isolation, as opposed to, for example, addressing undermethylation, optimizing zinc, decreasing activity at the NMDA and addressing sources of oxidative stress.Candida & MoldAside from undermethylation, low serotonin activity, and high activity at the NMDA receptor, those with OCD appear to have high oxidative stress, as is the case with most brain-related conditions. One of the more common sources of oxidative stress I see in my practice is candida overgrowth in the GI tract, which often follows antibiotic exposure and /or mold toxicity due to water damage causing seen or unseen toxic mold. Because mold and candida (yeast) thrive on sugar and a high-carb diet, symptoms can fluctuate with sugar or carb intake. How might candida and mold intersect with the NMDA receptor? Mold and yeast can contribute to high histamine states. Histamine can increase activity at the NMDA receptor. EstrogenFor women and teen girls that I see with OCD, there is often a fluctuation in their OCD symptoms with their cycle. Typically, their symptoms worsen during the times of the month when estrogen is the highest. This may be because estrogen can increase activity at the NMDA receptor.PANDAS & PANSWhen a child has an abrupt onset of OCD symptoms, PANDAS and PANS should be considered.* PANDAS = Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections* PANS = Pediatric Acute-Onset Neuropsychiatric SyndromePANDAS and PANS are autoimmune conditions, meaning the immune system is acting on the body, in this case, a part of the brain called the basal ganglia, that involves an acute onset of OCD symptoms. Other symptoms can include restricted eating, mood symptoms, regression in academic or social skills, and motor tics. While triggers are often viral, bacterial (strep in the case of PANDAS), candida,or other microbial source, what is underlying the dysregulated immune response to such microbes, in my experience, is mold toxicity. SummaryBecause OCD can be difficult to treat, my hope in sharing this information is to raise awareness that effective OCD treatments can require a multifaceted approach that includes:* addressing methylation (and high pyrroles if present) to improve serotonin activity* decreasing activity at the NMDA receptor* by optimizing zinc* using supplements or medication* addressing sources of inflammation and high histamine* address sources of oxidative stress - trauma, stress, toxins, inflammation If you find this information helpful and would like to help me get this out into the world, please consider sharing:As always, I welcome your comments, questions, and experience.Until next time,CourtneyP.S. To learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comMedical Disclaimer:This newsletter and podcast episode is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for yourself or others, including but not limited to patients you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 19m 29s | ||||||
| 1/27/25 |  Breakthrough Theory of Bipolar Disorder | This past week, I had the pleasure of attending the Advanced Course for Walsh-Trained Practitioners. To date, 1,200 practitioners from 75 countries have been trained using the Walsh approach.For those unfamiliar, the Walsh Research Institute, founded by Dr. William Walsh, has looked at the nutrient levels of over 30,000 people with brain-related symptoms and found a surprisingly small number of nutrient imbalances (low zinc, high copper, high pyrroles, and methylation imbalances) that repeatedly show up. We address these imbalances in those with depression, anxiety, panic, obsessions, compulsions, inattention, brain fog, hyperactivity, autism, dementia, psychosis, and mood swings with significant and, at times, dramatic results. Bipolar disorder, however, because of its shifting in neurotransmitter states from mania and depression, can be particularly difficult to treat. More than nine million Americans have been diagnosed with bipolar disorder. This severe condition can lead to drug or alcohol use, financial or legal problems, discord in relationships, work and school instability, and/or suicide attempts or suicide. The course typically begins with an acute onset, followed by episodes of mania and depression, which often worsens in severity over time.In this post, after describing bipolar disorder, I will use Dr. Walsh’s Comprehensive Theory of Bipolar Disorder, recently shared at the Society of Neuroscience, to explain:* the cause of bipolar disorder* the reason for the onset, persistence, and increasing severity for many over time* the reason for the increased risk of other health issues* the reason for the switch between manic and depressive states* how this information impacts treatment and preventionBipolar DisorderIt is important to note that the type of bipolar disorder I am referring to here is Bipolar I, a condition in which there are discrete episodes of mania often followed by episodes of depression. Such episodes can occur rarely or even multiple times a year.Manic episodes usually last a week up to several months and include three or more of the following:* increase in activity, energy, or agitation* distorted sense of well-being or self-confidence* needing much less sleep than usual* usually talkative or talking fast* racing thoughts or flight of ideas (jumping from one topic to another)* easily distracted* poor decision-making- e.g., excessive spending, risky sexual behavior* may become psychotic (have a break from reality)Hypomania has less severe symptoms which have less impact on functioning at work, school, social activities, and relationships. Having hypomanic episodes is not sufficient to warrant a diagnosis of Bipolar I.Depressive episodes, which often last a couple of weeks but can vary, include five or more of the below symptoms that are affecting functioning at work, school, social activities, and relationships:* depressed mood (sad, lacking feeling, hopeless, irritable, angry, or tearful)* marked loss of interest or enjoyment of activities* weight loss or weight gain (without dieting or overeating)* too much or too little sleep* behavior slowed down or restless* fatigue - loss of energy* feelings of worthlessness or inappropriate guilt* problems concentrating or making decisions* suicidal thoughts, plans, or attemptsBipolar II Disorder is a different condition. This diagnosis is given when someone has at least one major depressive episode and at least one hypomanic episode. Depressive episodes are often longer here. There is never a manic episode. Despite its name, this is not a milder form of Bipolar I. Biochemically, it is considered a different disorder.Rapid cycling is used to describe bipolar disorder when, in the past year, there have been at least four episodes of switching from mania or hypomania to depression. This can describe either type I or type II (depending on the presence or absence of mania). As with many other diagnoses, the terms came from seemingly related symptoms instead of a root cause or biochemical understanding.Dr. Walsh’s comprehensive theory, which I’ll describe, focuses on Bipolar I, in which there are manic episodes usually followed by depressive episodes. For those who struggle with mood swings changing within a day or a week as opposed to discrete mood episodes of mania or depression, pyrrole disorder should be considered.Genetics or Epigenetics?Having a first-degree relative (parent or sibling) with bipolar disorder raises the risk of developing bipolar disorder. After thirty years of genetic research, however, a gene for bipolar disorder has not been identified. The genetics are more complicated. It appears there are many genes involved.2021 Genome-Wide Association Study (GWAS)These studies compared the genomes of about 5,000 individuals with bipolar disorder and about 8,000 (controls/individuals without bipolar disorder). Over time, more and more “bipolar” genetic variants have been identified. By 2021, there were 64; however, there are expected to be hundreds. Of these 64 genetic variants, 49 are DNA repair genes and antioxidant genes that occur throughout the body (not just the brain). Just as it sounds, DNA repair genes make enzymes that repair DNA. Antioxidant genes make enzymes that support our protective antioxidant systems. Many of these genetic variants are also associated with cancer and other conditions impacted by DNA damage. This would suggest that those with bipolar disorder come into the world with a vulnerability in their ability to repair DNA damage (which translates to cell damage, tissue damage, and, in the case of the brain, neuronal damage. An event, however, is required to shift this vulnerability to illness.Accelerated DNA DamageWhat damages DNA? Free radicals and thus oxidative stress. To remind you, oxidative stress occurs when our body’s inherent antioxidant systems are overwhelmed or depleted by free radicals (due to an insult - a toxic exposure(s), source of inflammation, or trauma). A depletion of our protection leaves our cells and DNA vulnerable to further oxidative stress and damage. If we have variants on protective genes, then we can be even more vulnerable.Numerous studies have found high levels of superoxide, hydroxyl, and ONNO (peroxynitrite)free radicals in those with bipolar disorder.This vulnerability to DNA damage also explains why many with bipolar disorder have a higher risk of other health issues, including heart disease, breast cancer, multiple sclerosis, kidney failure, immune disorders, migraines, gastrointestinal illnesses, and others. But What About the Other 15 Genes? Genetic Weakness on Ion ChannelsThe remaining identified genes are more specific to bipolar disorder and relate to ion channel genes. Ion channels exist on the neuronal membranes, allowing potassium, sodium, and calcium to move in and out of the nerve cell. This movement creates an electrical charge that travels down the cell, releasing a neurotransmitter into the space between that neuron and other neurons to communicate with the next cell(s). OnsetHere again, an epigenetic event (toxic exposure, trauma, significant illness, etc.) leading to oxidative overload impacts the production of the proteins used in these channels, which affects the movement of ions in and out of the cell (more specifically causing flooding of potassium ions (K+) outside the cell) leading to hyperactivity of that nerve. This is why Dr. Walsh’s theory considers bipolar disorder a channelopathy.EuthymiaEuthymia - when the mood is neither manic nor depressed - interestingly, appears to be the first mood state after the onset of the condition. The flooding of K+ outside the cell leads to hyperactivity of neurons for serotonin. However, that doesn’t appear to cause symptoms since serotonin inhibits or keeps the activity of dopamine, norepinephrine, and glutamate in check.ManiaThe onset of mania starts to occur when the serotonin neuron hyperactivity (from the K+ flooding outside the cells) starts to fizzle out. What follows is a reduction in the inhibition of the neurotransmitters (dopamine, norepinephrine, glutamate, and others) that cause widespread neuronal hyperactivity, which causes manic symptoms.Eventually, the declining serotonin activity becomes the dominating force and triggers depression, which may persist for some time. Eventually, the serotonin nerves return to hyperactivity (again keeping things at bay), resulting in a stable mood - euthymia. Progression of Illness It is well known that preventing manic episodes can prevent the severity of the condition from escalating over time. Dr. Walsh’s theory also addresses why.Aside from impacting neurotransmission, the problems occurring at the ion channels are also associated with further DNA damage. This means that each episode can potentially add to the DNA damage. Add to this typical DNA damage (for all of us) that comes with aging. A typically untreated original and often persistent insult (such as a toxic exposure), events occurring at the ion channel, and aging can lead to the progression and increasing severity of illness.TreatmentAs with any theory, the inevitable question becomes, how does this impact treatment? Allopathic or mainstream psychiatry uses medication approaches that aim and usually succeed at stabilizing mood. Again, this is important because of the consequences of mania or depression but also because of the potential physiologic damage caused by ongoing episodes. What isn’t typically addressed in conventional psychiatry are:* Sources of oxidative stress. Does this person have mold toxicity, Lyme, metal toxicity, candida or other microbial overgrowth, chemical exposures, high EMF exposure, trauma, and/or chronic stress that are continuing to deplete protections and contribute to DNA damage? These are the types of issues that those of us who consider ourselves functional and environmental psychiatrists address.* Support for the antioxidant system. As with any brain condition, robust antioxidant support is indicated to address free radicals, but in this case, it is also indicated to prevent further DNA damage and to protect the ion channels. * Nutrient imbalances in varying combinations are typically also involved, such as methylation imbalances (often overmethylation), pyrrole disorder, and copper-zinc imbalances. Each of these can be exacerbated by high oxidative stress, which is a further cause of oxidative stress.Research into targeted antioxidants will be needed to build upon Dr. Walsh’s research. The free radicals (superoxide, hydroxyl ions, and ONNO) are more easily addressed in the body than in the brain. In the meantime, in addition to more typical antioxidants, NAC (which inhibits activity at the glutamate receptor) and MT (metallothionein) promotion therapy (a combination of glutathione, zinc, B6, and specific amino acids) are expected to be beneficial.PreventionBecause bipolar disorder appears to be an epigenetic DNA damage illness (caused by major oxidative overload), early antioxidant treatment in those who are vulnerable to bipolar disorder may prevent the onset and development of this disease. It won’t be long before such vulnerabilities can be identified, as early as infancy.For more on the work of Dr. William Walsh and the Walsh Research Institute Practioner Resource Map (, visit: https://www.walshinstitute.org/As always, I welcome your comments and questions.And if you would like to help me get this information out into the world, please consider sharing.Until next time,Courtney P.S. To learn more about non-patient consultations, treatment, and monthly mentorship groups, please visit my website at:CourtneySnyderMD.comMedical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for yourself or others, including but not limited to patients you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 17m 59s | ||||||
| 12/11/24 |  Understanding the Impact of Toxins on the Brain & Brain Development | Recently I saw a humorous reel of a man going through his day. As he does, you hear his inner dialogue. He’s trying to prepare a healthy snack, but at every turn, he’s stopped by his voice pointing out exposure to toxins - in the packaging, the water, the skin of the fruit. Eventually, he sits down and opens a bag of chips.Can we lower our exposure to toxins (and support detoxification) and not live in fear? I think we can. We can all hold this heavy topic lightly and do the best we can, knowing that there’s no perfection here.“If we are going to live so intimately with these chemicals, eating and drinking them, taking them into the very marrow of our bones - we had better know something about their nature and their power.” - Rachel Carson in “Silent Spring” (1962)In this episode, I'd like to help you better know something about the nature and power of the chemicals and heavy metals that we’re exposed to. I’ll discuss* The cumulative effects of our exposures* Sources of toxins* Oxidative stress* How toxins contribute to chronic health conditions, including psychiatric conditions* Impacts on the developing brain* How oxidative stress can be measuredTo learn more about the root causes of brain symptoms and the consultations that I offer, visit courtneysnydermd.comDisclaimer:This podcast is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for yourself or others, including but not limited to patients you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 16m 42s | ||||||
| 11/5/24 |  Understanding the Pineal Gland, Melatonin & Sleep | There is a wealth of information about sleep. In this podcast, I'll highlight aspects I find especially interesting and significant. * The Pineal Gland* The Seat of the Soul* Flouride* Melatonin* Creating Melatonin* Cortisol* Brain waves* Falling Asleep & Waking Up* REM (rapid eye movement) versus non-REM sleep* Sleep cyclesIn a future episode, I will delve into tools and techniques for optimizing sleep.To learn more about the root causes of brain symptoms and the consultations that I offer, visit courtneysnydermd.comDisclaimer:This podcast is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for yourself or others, including but not limited to patients you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 14m 55s | ||||||
| 10/31/24 |  Favorite Functional Medicine Psychiatry Books✨ | functional medicinepsychiatry+4 | — | — | — | functional medicinepsychiatry books+5 | — | 15m 03s | |
| 10/8/24 |  How Estrogen, Progesterone & Testosterone Impact Neurotransmitters✨ | hormonesneurotransmitters+4 | — | — | — | estrogenprogesterone+4 | — | 11m 47s | |
| 9/30/24 |  Limbic System Dysfunction & What We Can Do About It✨ | limbic systemamygdala+4 | — | Holistic Psychiatry Podcast | — | limbic systemamygdala+6 | — | 16m 06s | |
| 9/23/24 |  Addiction: Multiple Root Causes Aligning | “Addiction” - a compulsive, chronic, physiological, or psychological need for a habit-forming substance, behavior, or activity having harmful physical, psychological, or social effects and typically causing well-defined symptoms (such as anxiety, irritability, tremors, or nausea) upon withdrawal or abstinence.” Like other health conditions, addiction is multifactorial. It is the result of an alignment of root causes. In this newsletter, I’ll discuss:* Substance addiction and behavioral addictions* Why addiction is not simply about dopamine and why there are multiple addictive personalities* How & why we differ in our physiologic response to substances* Our culture’s shaming and punishment of addiction while fueling addiction* The role of attachment disruption, trauma, emotional dysregulation, and social isolationSubstance AddictionWhen it comes to addiction, you might expect me to talk a lot about dopamine. Not all substance addictions are the same, however. Opioids act very differently on the body than alcohol, which acts differently than cocaine. Some substances are more addictive than others, and even more so in certain people. For most people, marijuana is less addictive, while alcohol, cocaine, and opioids are more addictive. Addictive Substances:* Alcohol* Caffeine* Cannabis* Hallucinogens* Sedatives and Hypnotics/Anxiolytics* Inhalants* Opioids* Stimulants* TobaccoSeemingly, 10-20 % of people who try substances will have problems with addiction. Our genetic makeup and the expression of our genes will impact how we react to substances, just as they will affect how we metabolize specific medications or environmental toxins. We could, for example, have a weak enzyme that slows our metabolism of alcohol and results in our becoming more intoxicated more quickly. We may have high neurotransmitter activity that we’re trying to calm down with substances, or we may have low neurotransmitter activity and are taking substances or even carrying out certain behaviors that increase our neurotransmitter activity. Behavioral AddictionWhile we can become severely addicted to substances, we can also become addicted to behaviors or the feelings brought on by the behavior or anticipation of the behavior. Examples of Behavioral Addiction:* Food addiction* Sex addiction* Love and relationship addiction* Codependence is considered a relationship addiction in that relationships are often one-sided, emotionally destructive, or even abusive.* Exercise addiction* Body dysmorphic disorder* Health addiction* Shopping addiction* Gambling addiction* Work addiction* Video game addiction* Internet addiction* Smartphone addiction* Social media addiction* Porn addiction* News addiction* Information addiction* Self-harm addiction* Extremism is also felt to overlap with addictionWe can become addicted to anything that spikes the reward chemicals in our brains. If we’re not sure if we’re addicted, we can ask ourselves, “Is the compulsive behavior having negative consequences?”The severity of our addictions falls on a spectrum. I may not have a gambling addiction where I am putting myself at financial risk; however, I could be addicted to sugar, which I know negatively impacts my health, gives me brain fog and fatigue, and causes me to check out of my relationships, including my relationship with myself. Culture: Shame & Punishment The last thing that we need if we are addicted to a substance or behavior is shame and punishment. Our culture still tends to see addiction as a moral failing or even a sin that can be removed with punishment. This thinking leads to simplistic consequences such as rejection by family and friends and even imprisonment. The same happens with other forms of mental illness, but in this case, there is even less understanding, less compassion, more anger, and more disdain.Culture: Fueling AddictionMeanwhile, most of us are becoming more addicted - addicted to our cell phones, social media, divisive stimulating news and information. We have more information coming at us than we can process. Our brains are flooded with catecholamines as we stay in highly stimulated states. One of those catecholamines is dopamine, which will drive motivation and have us in pursuit of “more.” While there may be a type of pleasure in that pursuit, it’s not a joyful or even content type of pleasure. When we are in pursuit, we are not present in our lives. Many of us can barely process our moments, days, and lives in these modern times. For many, what was a life of memorable moments (positive and painful) has become a blur of days quickly passing by. Before we’ve had time to process what has happened, what we’ve experienced, or what we’ve felt, our minds are in pursuit of the next thing we need to know or have.With addictive technology comes the marketing and its messages - “more food, more sex, more youth and beauty, more health, more money, more success, and even more love - the elusive movie kind. We are forgetting how to be satisfied and tolerate uncomfortable feelings.Attachment & TraumaWe haven’t all had the same early attachment experiences. Some of us have experienced childhood trauma. We don’t know what safety feels like. Two-thirds of those with opioid addiction have childhood trauma. This doesn’t account for the trauma that can occur before verbal memory, which is usually not reported.Childhood trauma impacts our autonomic nervous system, our limbic system, and our hormonal stress response. Before we even experience a stressor, our baseline neurotransmitters may already be too high. Our trauma, in combination with our genetic variants, may result in high neurotransmitters that we may try to calm down with our addiction, or our trauma, in combination with our genetic variants, may have us seeking out stimulation so we can feel more alive and connected.Social IsolationPart of our understanding of addiction comes from the work of American psychologist Dr. Bruce Alexander, who did the “Rat Park” study. Previous research had already shown that when rats were put in solitary confinement and given a choice between water and heroin or cocaine, the rats repetitively consumed the drug-laced water until they overdosed and died.Alexander realized that the problem may not be the rats but the environment. Rats are social animals, just as we are. So, he created “rat parks,” where the rats could roam, play, socialize, and have sex. Despite being given the same access to the two types of drug-laced water, these rats preferred the plain water. Even if they did drink the drug-laced water occasionally, they never did obsessively, nor did they overdose. The social environment was protective against addiction. If we want to help those with addiction, we need to think about connection. If we want to help ourselves with an addiction, we need to think about connection.Emotional RegulationOur ability to regulate our emotions (increase calm and decrease fear and anger) comes through interactions with other humans - safe humans. Ideally, we learn to regulate our emotions during our first three years. When we were distressed as infants and toddlers, we communicated that distress through our cries and facial expressions, our caregivers responded, and our physiology returned to a sense of calm and safety. This repeated process - not necessarily perfect, but “good enough” - resulted in our internalizing that early relationship and, with that, an ability to recognize our feelings, trust others, feel worthy, respond to uncomfortable feelings with coping skills, and return to our baseline emotional state. Without this skill we acquire through attachment, we can become overwhelmed by our feelings or detached from our feelings. Our experiences, genetics, and temperament will impact which direction we go.There is not one “addictive personality” but many addictive personalities. Some of us will be highly sensitive, and others will have a low level of sensitivity. Some of us will become overwhelmed by stress or stimulation and use addictions as a way to try to calm our emotional and high neurotransmitter states. Others will seek sensory stimulation or risk-taking to bump those neurotransmitters and increase the feeling state. Of course, our biochemical differences impact this as well:* For those of us who are undermethylated, we may find that we are sensory seeking, have high activity at the NMDA receptor, and find ourselves craving whatever has come to have meaning or has left a mark on our neurophysiology. * For those of us who are overmethylated, we may have the desire to calm things down, slow our racing thoughts, and lower our high neurotransmitter activity.* For those of us with high pyrroles (and or CAPs profile), we may feel socially anxious or overstimulated and desire to feel calm and comfortable, but at other times, we may feel brave and invincible.“Being bold and adventurous and being sad and cautious seem like opposite personality types. However, these two paths to addiction are actually not mutually exclusive. The third way involves having both kinds of traits, where people alternatively fear and desire novelty and behavior swings from being impulsive and rash to being compulsive, fear driven, and stuck in rigid patterns. ……My own story spirals around this paradoxical situation: I was driven enough to excel academically and fundamentally scared of change and of other people—yet I was also reckless enough to sell cocaine and shoot heroin.” - Maia Szalavitz We need to think more broadly about addiction, just as we would any other health condition. We need to address the underlying physiological root causes, meet our human need for connection, and learn ways to experience, tolerate, and cope with our very human and necessary feeling states. In this week’s paid newsletter, I look forward to discussing cases to illustrate how various neurotransmitters can be at play with different substance addictions and how targeted nutrients can be used in the treatment of addictions - both substance and behavioral. Until next time,CourtneyCourtneySnyderMD.comIf you’d like to dive deeper into the root causes of brain symptoms, consider becoming a paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 13m 05s | ||||||
| 9/17/24 |  Physician Depression, Burnout & Suicide - Consider Undermethylation✨ | physician depressionburnout+4 | — | courtneysnydermd.comcourtneysnydermd.substack.com | — | physician mental healthburnout+5 | — | 14m 48s | |
| 9/2/24 |  Mold Prevention For Brain Health - Home Exterior Maintenance | “Exterior building maintenance is crucial for preventing mold from growing inside a building” - Jerry Parker, CEIC, CMRTwenty-five percent of people appear to be susceptible to mold toxicity - a surprisingly common cause of brain symptoms, including brain fog, fatigue, depression, anxiety, mood swings, OCD, panic, and psychosis. Mold toxicity can also be an underlying factor in pyrrole disorder, candida, and copper-zinc imbalances, which also cause brain symptoms. Mold toxicity should also be considered when there are new-onset mental health issues in college students exposed to mold in their dorms or apartments.Many chronic physical health issues can result as well, including autoimmune conditions. In my experience, mold toxicity is the most common cause of mast cell activation.Jerry Parker is a Certified Indoor Environmental Consultant (CIEC) and Certified Microbial Remediator (CMR). Jerry has been helpful to me personally and professionally and has taught me a great deal about the environmental aspects of mold. Jerry owns Environmental Solutions Group, LLC, which has served residential and commercial clients for the last twenty years. He is about to launch an educational and consulting platform, 4 Indoor Air Quality LLC.In this newsletter and podcast, Jerry and I discuss:* why mold prevention isn’t just about keeping water out; it’s also about moving water away from the foundation* ways to ensure rainwater is moving away from our home and its foundation * landscaping and vegetation* gutters and downspouts* roof and siding integrity* chimneys* cantilever fireplaces and bay windows* doors and window sealing* siding and deck attachment* the importance of regular self-assessmentsAt a later date, Jerry and I will discuss mold prevention with a focus on the interior of our homes.Let us know if you have any questions or comments on mold prevention (exterior or interior).Have a good week,CourtneyCourtneySnyderMD.comTo contact Jerry Parker CIEC, CMR: email - info.4IAQ.com 4IAQ.comRelated Content:* Mold Toxicity: Depression, Anxiety, Brain Fog & Fatigue (free)* Mold Toxicity & the Brain (free)* Mold & Candida in the Brain (paid)* Environmental Mold Myths (paid) This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 57m 28s | ||||||
| 8/26/24 |  What Skin Symptoms Can Tell Us About Brain Symptoms✨ | skin symptomsbrain health+4 | — | — | — | skin conditionsbrain symptoms+6 | — | 10m 14s | |
| 8/12/24 |  Smart Meters, Brain Symptoms & Solutions | Eric Windheim, BA, BBEC, EMRS, RFSO is a Certified Electromagnetic Radiation Specialist and Certified Building Biology Environmental Consultant. He is the founder of Windheim Solutions, which provides inspection, testing, and remediation of problematic EMFs. In this episode, we discuss smart meters, which are digital devices that measure electricity usage in real-time, and wirelessly send that information to the utility company. Smart meters are sometimes used for gas and water.Though there are four harmful types of electromagnetic fields—radiofrequency (wireless), electric fields, magnetic fields, and dirty electricity—smart meters use radio frequencies.Brain symptoms associated with EMF exposure include insomnia, memory problems, irritability, depression, personality changes, inattention, fatigue, confusion, headache, ringing in the ears, dizziness, numbness, and tingling.Problematic EMF can impact the brain in many ways. It causes oxidative stress and neurotoxicity. It disrupts our immune system, innate electricity, hormones, microbiome, limbic and autonomic nervous systems, and the blood-brain barrier. EMF can also contribute to elevated blood sugar.The good news is that there are many ways we can lower our exposure.In this newsletter:* Eric shares: * How he became an electromagnetic radiation specialist.* The story of smart meters * His role in a national victory with Sacramento Municipal Utility District, the first municipal electric utility to allow customers to regain the use of analog meters. * We discuss the following questions:* How do you “opt-out” and return to an analog meter?* What can you do if you have to have a smart meter?* What can you do if you’re getting radio frequency exposure from your neighbor’s smart meters or other wireless devices?* What meter can measure radio frequencies in and around your home?* How can you find an electromagnetic radiation specialist?If you’d like to join the conversations, consider sharing your experience or questions.Have a good week,CourtneyCourtneySnyderMD.comMentioned Resources* Windheim EMF Solutions* WIndheim EMF Solutions Youtube Channel* Building Biology Institute* EMF & the Brain* Electromagnetic Hypersensitivity - A Lesser Known Root Cause* How We Can Start to Assess & Lower Our EMF Exposure This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 46m 21s | ||||||
| 7/29/24 | 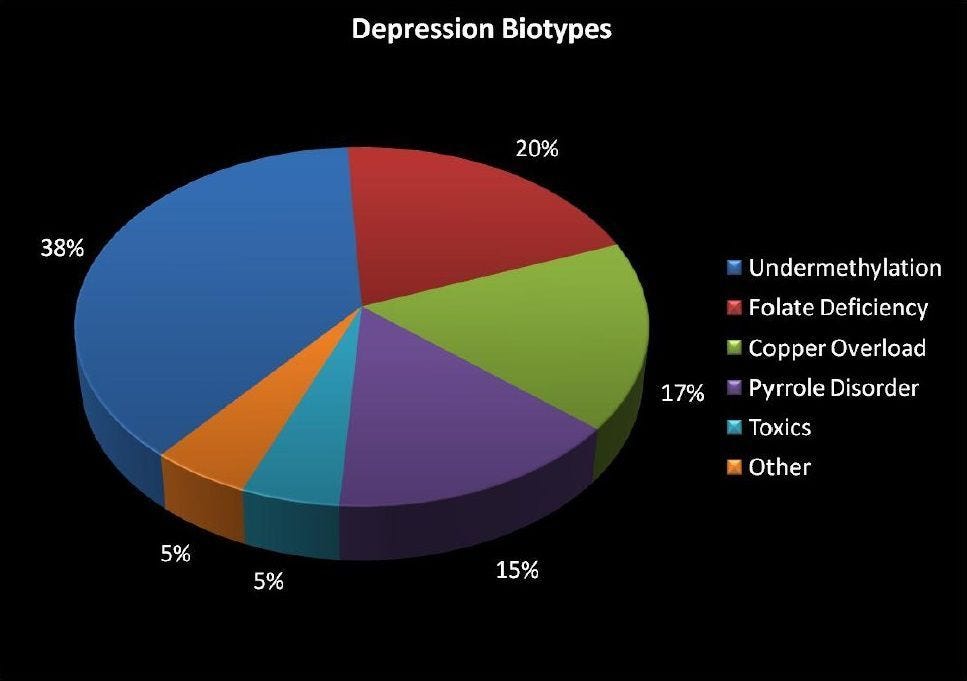 Walsh Biotypes of Depression With a Focus on Undermethylation | I recently had the pleasure of being on the Nourished By Nature: Mind Body Wellness Podcast with Annika Taylor, a holistic health practitioner. After sharing with Annika how I became a holistic psychiatrist and how I define holistic psychiatry, we discuss:* The Walsh Research Institute’s data on nutrient levels of 30,000 people with brain-related symptoms, and what were found to be the most common imbalances (One or more of these imbalances is present in about 90-95% of the patient's that I evaluate for brain-related symptoms).* The Walsh biotypes of depression. How I test for the copper-zinc imbalances, pyrrole disorder, and methylation imbalances.* High copper and its relationship to ADHD, anxiety, depression and post-partum. depression, anxiety and psychosis.* Pyrrole disorder - symptoms, traits and treatment.* How methylation impacts brain health.* Under and over-methylation symptoms and traits.* Treatment of under-methylation.* How this understanding can remove the stigma associated with mental health conditions, and provide healing and hope.In recent years, Dr. Walsh discovered that undermethylation is increasing in the population while overmethylation is decreasing.If you’d like to add to the discussion, I always appreciate your questions and comments.Have a great week,CourtneyRelated Resources:Annika Taylor - nourishedbynature.comWalsh Research InstituteFor links to specific topics address see links in the description above. Medical Disclaimer:This newsletter is for educational purposes and not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment for yourself or others, including but not limited to patients you are treating (if you are a practitioner). Consult your physician for any medical issues that you may be having. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 43m 36s | ||||||
| 7/22/24 |  Effective Prevention & Treatment of Alzheimer's | Because Alzheimer’s starts before the onset of symptoms and because having almost any psychiatric condition appears to raise our vulnerability, many of the tools mentioned here relate to other brain symptoms and conditions as well.“What we call Alzheimer's disease is actually a protective response to a wide variety of insults to the brain: inflammation, insulin resistance, toxins, infections, and inadequate levels of nutrients, hormones, and growth factors.” - Dale Bredesen, MD (The End of Alzheimer’s Program: The First Protocol to Enhance Cognition and Reverse Decline at Any Age)In this newsletter, I’ll discuss:* Medications used in mainstream medicine * Lifestyle and functional medicine approaches to preventing and treating Alzheimer’s* Feeding the brain - The ketogenic diet and intermittent fasting* Exercising the body and brain* Sleep and sleep apnea* Hormonal deficiencies and dysregulation* Oral health* Toxicity, depletion of antioxidants and oxidative stress* Brain inflammation If you have any questions or comments (or topic suggestions),…If you know someone who may benefit,…Have a great week,CourtneyResources mentioned:* Precision Medicine Approach to Alzheimer’s Disease: Successful Pilot Project* Reversing Alzheimer’s: The New Toolkit to Improve Cognition and Protect Brain Health by Dr. Heather Sandison * The End of Alzheimer’s by Dale Bredesen, MD* Walsh Research InstitutePrevious newsletters/podcast episodes mentioned:* Alzheimer’s: Factors We Have Control Over* Regulating Blood Sugar For the Brain* Intermittent Fasting & the Brain* Exercise & the Brain * Oxidative Stress & the Brain* Lowering Brain Inflammation This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit courtneysnydermd.substack.com/subscribe | 19m 57s | ||||||
Showing 25 of 72
Pitch Fit is a Pro feature
See how bookable this show is for guests, which brands already advertise, the per-episode ad value, and the best-fit guest and sponsor profile. The numbers are blurred on the free plan.
How readily this show books outside guests like you.
How proven this show is for host-read sponsorships.
For Guests
ProFor Advertisers
ProUpgrade to Pro to unlock guest cadence, sponsor categories, fit scores, and per-episode ad value for this show.
Chart Positions
1 placement across 1 market.
Chart Positions
1 placement across 1 market.