
Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Most discussed topics
Brands & references
Est. Listeners
Insufficient chart data. Estimates will improve as the show charts.
- Per-Episode Audience
Est. listeners per new episode within ~30 days
N/A🎙 Daily cadence·79 episodes·Last published today - Monthly Reach
Unique listeners across all episodes (30 days)
N/A - Active Followers
Loyal subscribers who consistently listen
N/A
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
From 15 epsHost
Recent guests
No guests detected in recent episodes.
Recent episodes
Alzheimer's and Amyloid 5: The Big Mistake
Jun 26, 2026
18m 30s
Alzheimer's and Amyloid 4: The Long Mistake
Jun 17, 2026
29m 51s
Alzheimer's and Amyloid 3: The Mistake of the Invisible Friend
Jun 10, 2026
29m 25s
Alzheimer’s and Amyloid 2: Mistakes Of Mice and Men
Jun 3, 2026
22m 34s
Alzheimer's and Amyloid Part 1: The First Mistake
May 28, 2026
20m 56s
Social Links & Contact
Official channels & resources
Official Website
Login
RSS Feed
Login
| Date | Episode | Topics | Guests | Brands | Places | Keywords | Sponsor | Length | |
|---|---|---|---|---|---|---|---|---|---|
| 6/26/26 |  Alzheimer's and Amyloid 5: The Big Mistake | In part 2 of this series I described a trial in which researchers developed a novel vaccine for Alzheimer’s patients, designed to rid the brain of amyloid. The vaccine worked, clearing amyloid—but their dementia progressed, unabated. This was, in other words, a full debunking of any notion that amyloid plaques are the cause of Alzheimer’s and that removing them can cure the disease.Interestingly, in a 2008 follow-up report on the study, a curious turn of phrase caught my eye: Do you see it? Did you feel the tectonic shift?In a single sentence the authors both tout their success with “disease modification,” and concede that removing amyloid didn’t help people. In other words, the ‘disease’ was not memory loss or crippling cognitive decline. It was amyloid. Which they ‘modified’. The operation was a success—but the patient died.RT is fully reader-supported. To keep doing it, I need help. Please consider paying for a subscription.Lest you believe this kind of language is isolated or antique, this week’s Journal of the American Medical Association, the worlds most circulated medical journal, includes an article about Alzheimer’s, with a review of the history of amyloid targeting. In it the author, an NIH neuroscientist, describes the anti-amyloid drug Aduhelm as “the first ever disease-modifying drug,” while acknowledging that it failed to help people. He also describes the two recent anti-amyloid drugs as beneficial, and ends with a breathless look to the future of amyloid research.Why should this language matter? Here is why: Incredibly, this 2024 NY Times article describes a study of a novel blood test for brain amyloid. Not for dementia. Or cognitive decline. Or human suffering. In other words, not for Alzheimer’s Disease—not as it is experienced by people—but for amyloid. Yet, the headline calls it ‘Alzheimer’s’.This is where decades of amyloid-centered thinking inevitably led. It began with the identification of brain amyloid, moved to the invention of highly specialized PET scans to see amyloid, and culminated in a blood test whose only purpose is to detect fragments of the amyloid seen on PET scans. The new blood tests are therefore not tests for Alzheimer’s disease. They are tests for amyloid, which they detect readily. And that is why they constantly miss Alzheimer’s when it is truly present, while labeling people with Alzheimer’s who don’t have it. (For the numbers, check out my 2024 piece).The test, in other words, fails miserably to identify Alzheimer’s Disease, because amyloid and Alzheimer’s are not the same thing.The distinction may seem trivial, but it represents one of the most consequential shifts in modern medicine. For more than a century, Alzheimer’s was a human condition: progressive loss of memory, reasoning, language, independence, and ultimately self. It was a disease experienced by patients and families.Amyloid was just one proposed explanation. But when it repeatedly failed, something happened: Rather than abandon the explanation, the field redefined the disease.The question quietly changed from ‘Does this person have Alzheimer’s dementia?’ to ‘Does this person have amyloid?’Everything else followed naturally.PET scans no longer needed to identify dementia—just amyloid. Blood tests no longer needed to predict who would lose their memory, they only needed to detect amyloid. Drugs no longer needed to help people, they had to remove amyloid.The microscope, the scanner, and the laboratory, all quietly replaced the patient.This is the Big Mistake, the same mistake that medicine repeatedly makes. In cholesterol, LDL gradually became more important than survival, or quality of life. In orthopedics, MRI abnormalities became more important than pain, or function. And now, in Alzheimer’s, amyloid became more important than dementia.People want to live longer and better, while doctors aim to seek pathology and diagnose disease. Doctors, and by extension the medical establishment, fail most tragically when they forget to put people first. Disease is not what appears on a PET scan, or an MRI, or in a cholesterol test, or under a microscope, or in a test tube. Disease is what happens to people.When medicine forgets that distinction, it treats pathology, not patients. And that is how Alzheimer’s gradually ceased to mean dementia, and came to mean amyloid.That is the Big Mistake.Next week we’ll talk about how intelligent, compassionate physicians can be swept up by pathology what it all means, and how you can avoid the traps that have been laid by a multi-industry machine carefully crafted to profit from the Big Mistake. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 18m 30s | ||||||
| 6/17/26 |  Alzheimer's and Amyloid 4: The Long Mistake | Over the first three parts in this series we followed the rise and fall of the Amyloid Hypothesis.The plaques failed. The idea of toxic precursors failed. The most influential oligomer paper in the field was ultimately retracted. By any ordinary standard of scientific reasoning, this should have marked the end of amyloid as a central explanation for Alzheimer’s Disease.Instead, something remarkable happened: As the scientific case for amyloid weakened, the clinical investment in amyloid accelerated.Drug companies continued developing anti-amyloid therapies. Regulators continued evaluating them. Researchers continued measuring amyloid. Billions of dollars flowed into a treatment strategy increasingly disconnected from the evidence.The result was the modern anti-amyloid drugs. What follows is two short essays I wrote about the clinical trials that won FDA approval for two of them. In both cases drug makers quite literally designed the trials to prove that the drugs DON’T help people with Alzheimer’s, apparently with full confidence that they could spin the results to suggest the opposite. It is among the most brazen examples of FDA game theory, and snake oil sales, that I can recall in decades of reviewing FDA trials.New Alzheimer’s Drugs Are Bringing Back the Wrong MemoriesApr 03, 2024I remember when, in 1999, the FDA approved Vioxx, a pain reliever that went on to kill an estimated 50,000 Americans. According to whistleblowers the FDA not only had the data to prevent the tragedy, they obstructed the investigation.I also remember the inspiring story of Frances Kelsea, an FDA physician who in 1960 refused to approve thalidomide despite approval in dozens of other countries, and industry pressure. The drug caused over 10,000 birth defects worldwide, but just 17 in the US where it was never approved.Now, in 2024, the FDA is on the verge of approving a third Alzheimer’s Disease drug. The first was Aduhelm in 2021, the second was Leqembi, in 2023. Donanemab, the third, is under review. The three are extremely similar. They’re all monoclonal antibodies, they all reduce amyloid plaques in the brain, and they all don’t work.In the 1980s researchers discovered amyloid plaques were associated with Alzheimer’s, spawning the ‘amyloid hypothesis’. If the plaques cause cognitive decline, it was hoped, removing them may slow or even reverse Alzheimer’s.Unfortunately, the theory has been dashed. First, studies show many with Alzheimer’s have no brain amyloid. Second, scientific reviews show at least 72 anti-amyloid agents have been researched, and none have worked. This includes nine monoclonal antibodies, a class that has failed so miserably and consistently a 2021 meta-analysis announced “the time has come to divert therapeutic efforts away from AAB [amyloid] immunotherapy.”Abject failure is certainly the case for Aduhelm. Two FDA studies were halted early for futility, and an expert panel voted 9-1 against approval (the FDA approved it anyway). Meanwhile, Leqembi ‘slowed cognitive decline’ by just 0.45 points on an 18-point scale, less than half the 1-point minimum deemed meaningful. Finally, the donanemab trial used a 144-point scale and reported a 3-point edge, well below the 9-point minimum determined by the company’s own research.These failures highlight a crucial distinction: statistical versus clinical differences. Studies often find a ‘statistical’—meaning mathematically identifiable—difference between groups. But research is a human task and thus inherently biased, so trial results commonly lean toward the drug. Particularly in large trials (the Alzheimer’s trials enrolled thousands) this often leads to a ‘statistical’ difference.But a clinical difference affects people’s lives. Which is why there are thousands of studies examining and meticulously defining the ‘minimal clinically important difference’ for scales like those in the Alzheimer’s trials. Those studies tell us the ‘differences’ in the antibody drug trials were so small that people with the disease, their families, and their doctors, would literally never notice them. In other words, they’re not real differences.Another issue may also be confusing starry-eyed loyalists. The drugs removed amyloid plaques quite effectively—a finding that closes the door on the amyloid hypothesis. Vanquishing amyloid plaques didn’t help people with Alzheimer’s.The chicanery of parading differences well below the thresholds for true benefit is happening now for a reason: We’re heading into a perfect storm of potential profit for AD drugs. Nearly 7 million in the US have symptomatic Alzheimer’s, with an expected doubling by 2050. This will likely balloon with the use of new, flawed blood tests that severely over-diagnose Alzheimer’s. And the drug, given through IV infusions, costs nearly $30K per year (not including infusion costs, facility fees, and other charges).A final tidbit: The drugs cause brain swelling, headaches, confusion, and occasionally death—in huge numbers. Donanemab, the latest, caused 24% of people’s brains to swell, while another 9% suffered infusion reactions. That’s 1 in 3 people seriously harmed by the drug, and zero helped. What’s worse, as noted in these pages, one can always expect the harms to be greater and the benefits smaller than reported in trials.As the FDA wrestles with the amyloid drugs, it seems natural to remember the agency’s heroic performance on harmful drugs of the past. But an effective Alzheimer’s treatment would bring back different memories.Why the Alzheimer’s Drugs Won’t Make Your Burger BetterFeb 04, 2025I like a burger. With cheese. And lettuce and tomato and maybe onion and ketchup or sauce (house choice). I prefer it rare. Really rare. Like, true blue.This last part is the downfall of many a burger joint where, fearing liability, kitchens won’t make a rare burger. To me, besides corrupting its taste, this means dubious beef. Sushi, steak tartare, and raw bar items are much riskier than anything cooked, but they’re still common menu items. A kitchen that won’t make a rare burger doesn’t trust its sourcing and prep for burger meat. Sad!But crucially, rare burgers aren’t just hard to find, they’re also tricky to make because they must—MUST—be seared on the outside and lightly cooked on the inside. This delicate contrast, a pillowy but juicy inside with a firm outer layer, is the mouth-watering soul of a great burger.So for home burgering, I got a meat thermometer.To my surprise, the first time I used it the reading was 122.68°. Impressive precision! But this number was, as the kids say, TMI (not to mention sus). Because while my gifted palate is a wonder of epicurean virtuosity, I cannot tell a 1° difference in temperature, much less 0.01°. Those decimal points are not helping me.I can tell rare from medium-rare (I think). That’s about 10° different. Which means somewhere between 1° and 10°, for me, the difference becomes perceivable and thus potentially meaningful. If I was bored and curious I might experiment to find the threshold, and in research parlance we would call it the ‘clinically significant’ difference. This principle, also known as the minimal clinically important difference (or ‘MCID’), defines the smallest improvement patients and doctors are able to perceive, a starting point for judging whether treatments provide a meaningful benefit.Curiously, however, all three FDA-approved Alzheimer’s drugs were tested in studies that are the equivalent of a 2-decimal point thermometer.Each trial enrolled way more people than needed to find improvements in dementia. Why? Because the more participants, the smaller a difference a study can find. But my thermometer, for instance, can detect differences that are much too tiny to matter. And so can studies. In research this is called over-powering, but in trials it’s very unusual. After all, genuinely helpful drug effects, even lowly MCIDs, aren’t tiny. So why would researchers go looking for tiny differences? Who even has the money and resources to enroll way too many people in a randomized trial??Oh. Wait.As discussed in these pages before, a jarring attribute of the Alzheimer’s drugs is that trials proved they do not make a perceivable difference. One hapless employee at Eli Lilly even spent years studying (and writing at least seven reports) to establish the MCID for cognitive impairment. He found it was at least 5 points on a 144-point scale for mild disease and 9 points for early Alzheimer’s. But his company’s drug Kisunla produced scores within 3 points of a placebo—in other words, indistinguishable from placebo. Meanwhile Biogen and Eisai’s drug Leqembi was within 0.45 points of placebo on an 18-point scale—also less than half the established MCID of 1 point.How could this happen? Were the studies purposefully over-powered? Or did they stumble upon tiny differences while seeking meaningful ones?In the Kisunla report Eli Lilly says they aimed to find a 3-point difference (!!!). The authors calculated that 1,000 participants would give them a 95% chance, or ‘power’, to find it. So they enrolled 1,000 people. Then they enrolled 736 more.What about Leqembi? The FDA approval trial also, amazingly, targeted 0.4 points better than placebo (!!!). This, they found, required 1,566 participants—and they enrolled nearly 1,800.This is over-over-powering. The original plans were over-powered, and then each study ADDED extra enrollments. These are confessions, hidden in plain sight in the methods sections of the papers, and they mean the companies knew before the trials started that their drugs don’t help. So they targeted statistical—not perceivable—differences, then convinced the FDA to approve the drugs.1Bonus question: How could the companies feel confident the studies would generate a statistical advantage for their drug? Answer: The double-dog placebo.In their brilliant, deeply researched investigation Jeanne Lenzer and Shannon Brownlee describe a woman who was convinced, and whose friend was convinced, Leqembi was rapidly improving her memory. But she was receiving a placebo. As placebo researcher Irving Hirsch explains in his wonderful book, placebo effects are common, but they’re reliably larger when people experience drug side effects. Side effects effectively unblind study participants, letting them know they’re on a real drug and amplifying their expectations, excitement, and thus placebo effects.One of the great ironies of modern scientific rigor, therefore, is that ineffective drugs in double-blinded trials can generate statistical advantages if they have harmful side effects. People given Leqembi in trials had infusion reactions 19% more often than those given placebos, and brain swelling 11% more often. That’s a lot of unblinding, easily enough double-dog placebo to virtually guarantee an advantage.2My burger thermometer gives me too much information, and so did the trials for the new Alzheimer’s drugs. Deliberately over-powered trials are a smoking gun, telling us what the companies knew all along: Their drugs don’t work.The story of the anti-amyloid drugs is often presented as a story of disappointing results. Placed within the chronology of amyloid research they are better described as a story of entirely predictable results.By the time these drugs entered clinical trials, the Amyloid Hypothesis was decimated. Plaques did not track with disease. Dementia could appear before plaques. Removing plaques did not stop dementia. The proposed replacement—the Amyloid Precursor Hypothesis—fared no better, collapsing under a combination of failed replication, failed trials, and outright fraud.The drug trials therefore did not rescue the theory. They confirmed its failure.This is why the central mystery of the Alzheimer’s story is not scientific, it is etiologic: How did this happen and why?If the plaques failed, why did amyloid remain the target? When the precursors failed, how could amyloid still be of interest? If removing amyloid then failed to help patients, why are we still chasing it?The answer lies in one of the most successful acts of disease redefinition in modern medicine.Next time we’ll examine the blood tests, PET scans, and diagnostic criteria that transformed amyloid from a failed explanation into the disease itself. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 29m 51s | ||||||
| 6/10/26 | 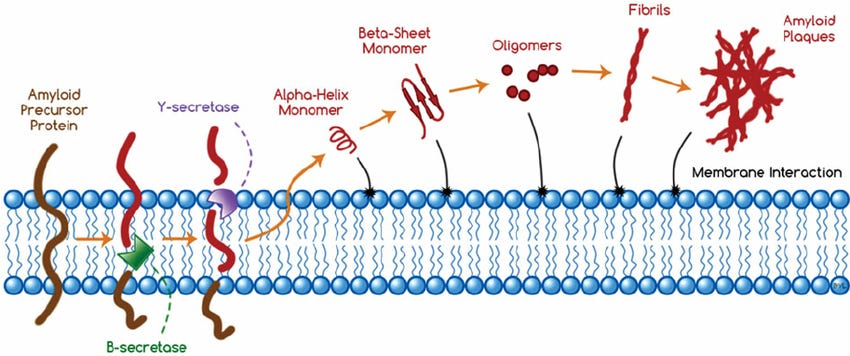 Alzheimer's and Amyloid 3: The Mistake of the Invisible Friend✨ | Alzheimer's diseaseAmyloid Hypothesis+3 | — | Alzheimer’sAmyloid Hypothesis+4 | — | Alzheimer'sAmyloid plaques+4 | — | 29m 25s | |
| 6/3/26 |  Alzheimer’s and Amyloid 2: Mistakes Of Mice and Men✨ | Alzheimer's Diseaseamyloid plaques+4 | — | University of Minnesotapharmaceutical industry+1 | — | Alzheimer'samyloid+6 | — | 22m 34s | |
| 5/28/26 | 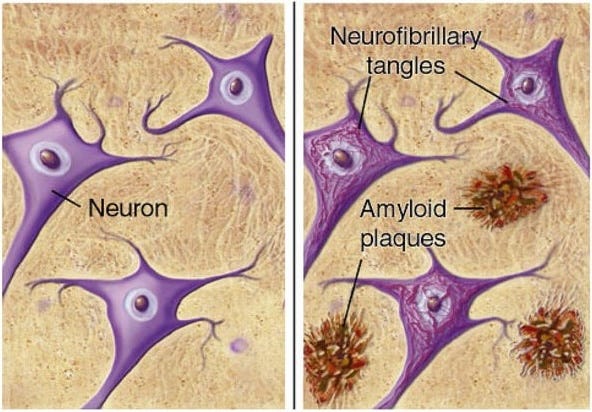 Alzheimer's and Amyloid Part 1: The First Mistake✨ | Alzheimer's researchAmyloid+3 | — | The Price is Right | — | Alzheimer'sAmyloid+3 | — | 20m 56s | |
| 5/20/26 | 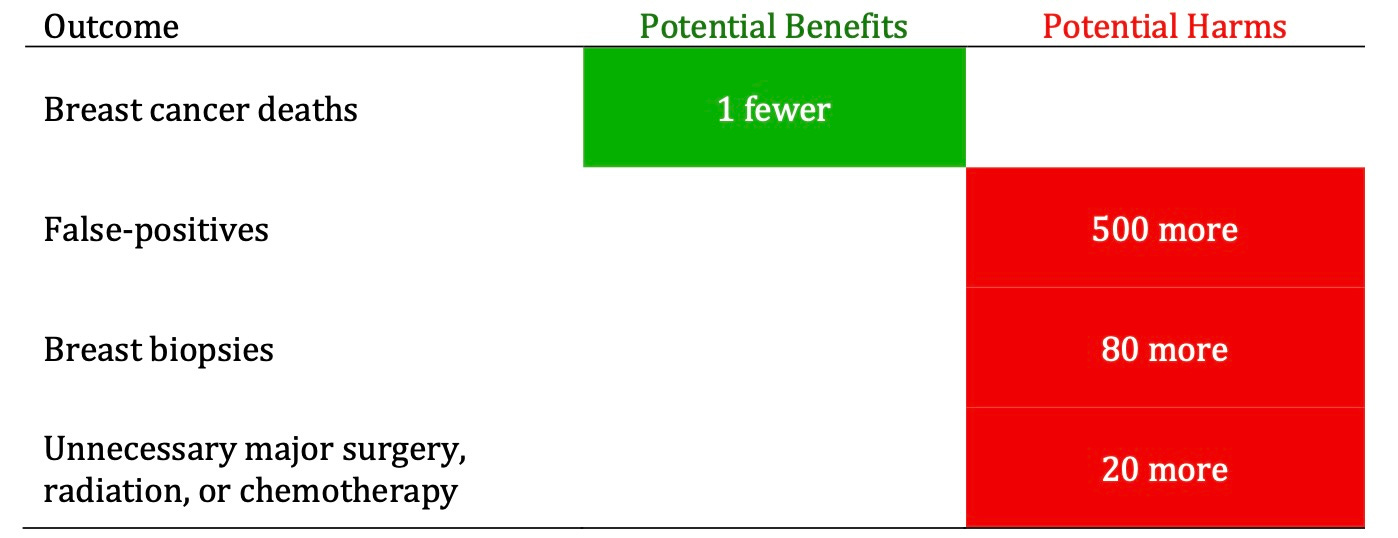 The Ghost On the Balance Sheet of Cancer Screening✨ | cancer screeningall-cause mortality+3 | — | HeartSaver 3000PSA+3 | — | cancer screeningall-cause mortality+6 | — | 33m 50s | |
| 5/12/26 | 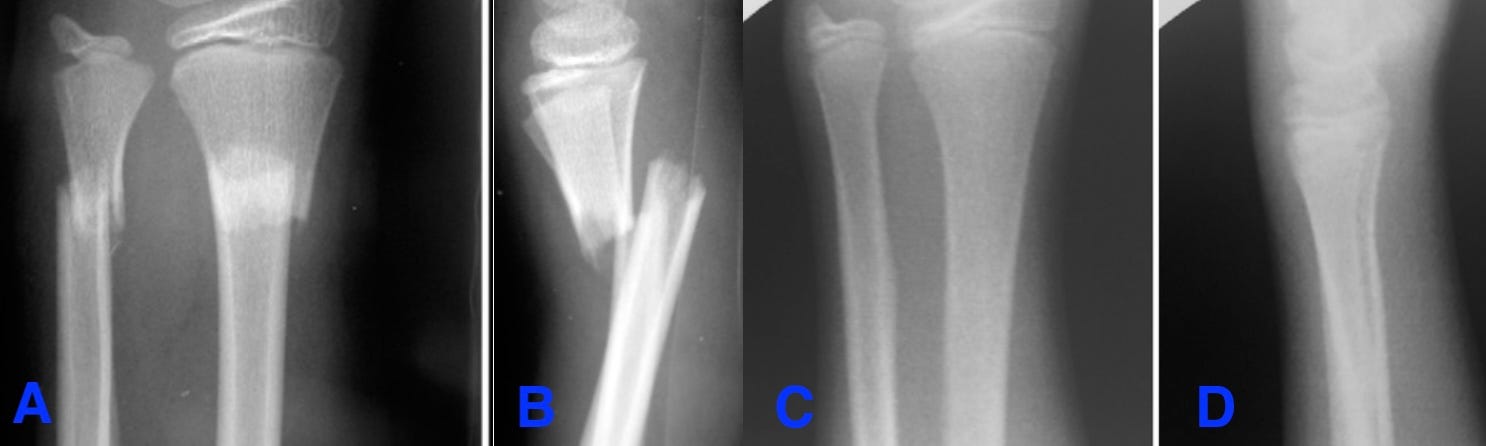 Surgery To Treat Knee Degeneration Increased Knee Degeneration✨ | knee degenerationorthopedic surgery+3 | — | Research TranslationU.S. | — | knee surgerydegeneration+3 | — | 24m 15s | |
| 5/7/26 | 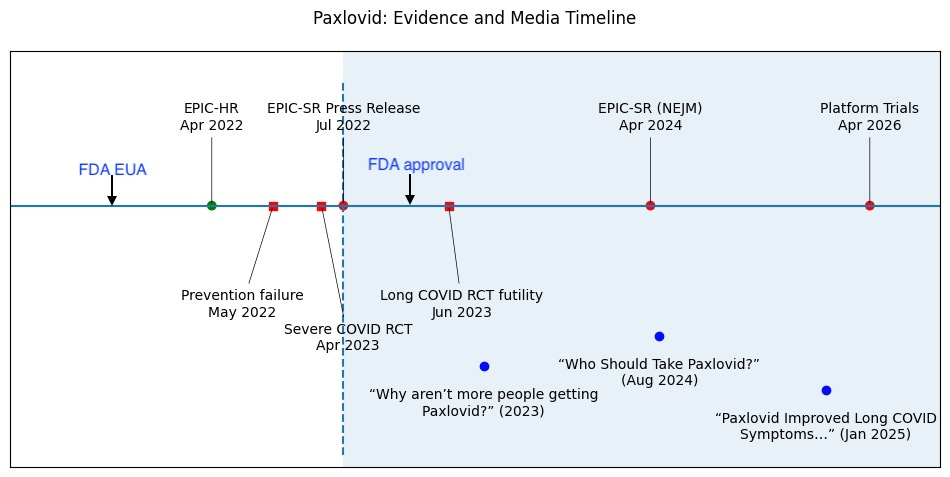 Paxlovid: A Requiem✨ | PaxlovidCOVID-19+4 | — | PaxlovidPfizer+1 | — | PaxlovidPfizer+5 | — | 30m 15s | |
| 4/29/26 | 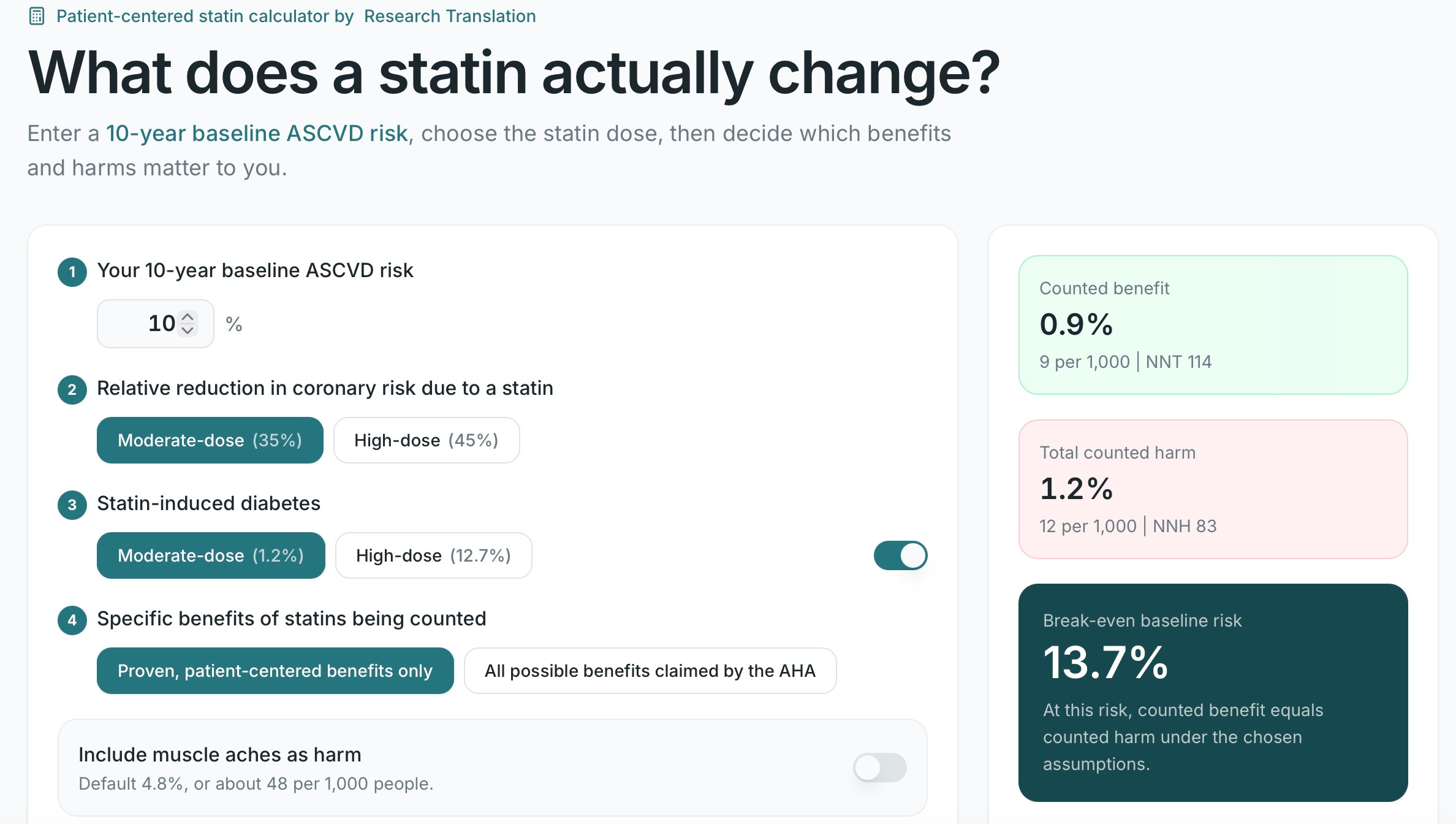 Cholesterol 5: The Power at Your End of the Stethoscope✨ | cholesterolmedical dogma+4 | — | AHACholesterol Mistake+1 | — | cholesterolLipid Hypothesis+5 | — | 13m 40s | |
| 4/22/26 | 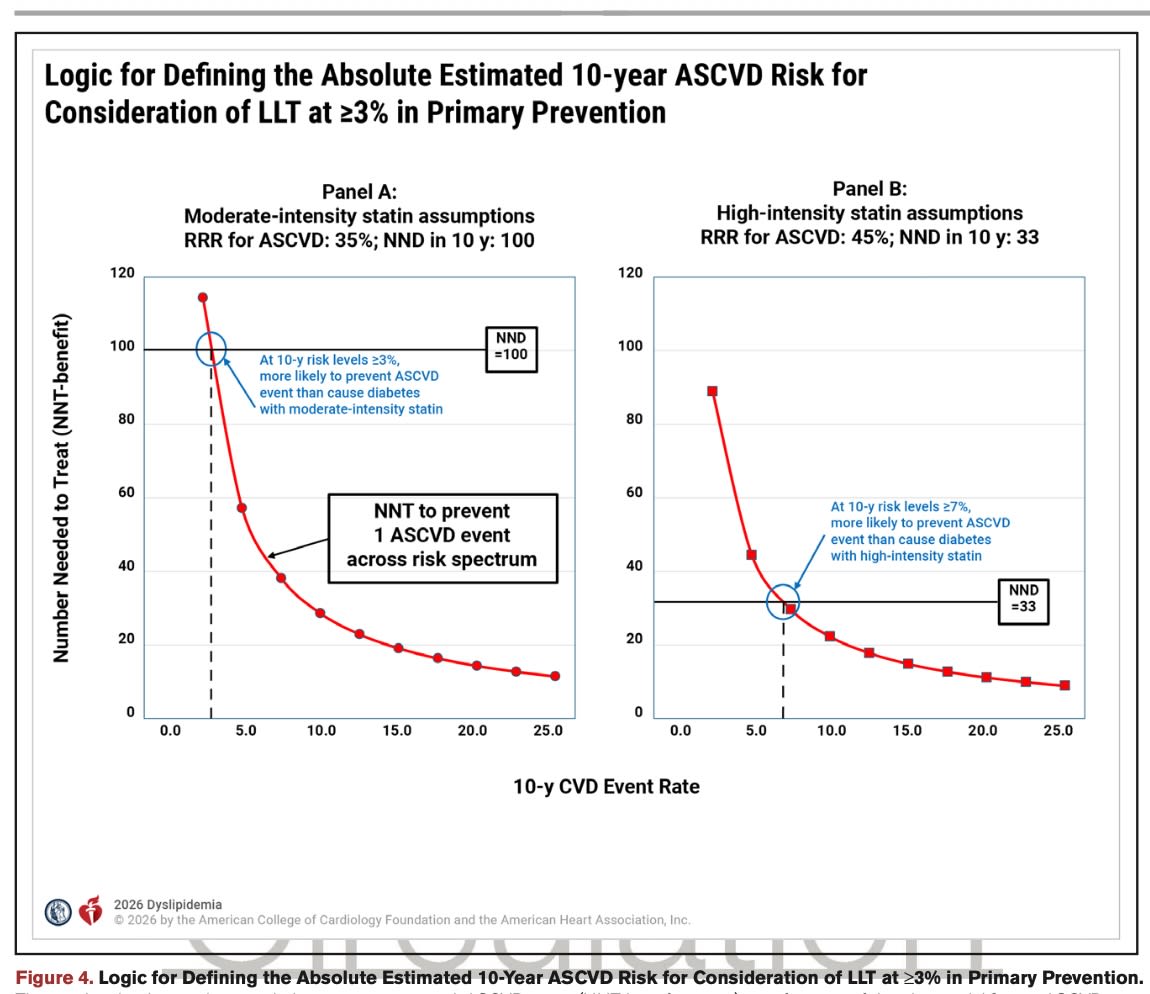 Checking The Math in New Statin Guidelines✨ | statin guidelinescholesterol+3 | — | dilaudidAHA | — | statincholesterol+3 | — | 44m 54s | |
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 4/16/26 |  Cholesterol 4: What Went Wrong✨ | cholesterolmedical misunderstanding+4 | — | WOSCOPSLipid Hypothesis | — | cholesterolLipid Hypothesis+4 | — | 21m 39s | |
| 4/9/26 |  Cholesterol 3b: A Study Straight Out Of Central Casting✨ | cholesterol researchheart disease+3 | — | New England Journal of MedicineAHA | — | cholesterolheart disease+5 | — | 19m 58s | |
| 4/8/26 |  Cholesterol 3: The Big Mistake✨ | cholesterolstatins+3 | — | statinsAHA | — | cholesterolAHA guidelines+3 | — | 38m 03s | |
| 4/1/26 |  Cholesterol 2: Cardiology's Nonfatal Mistake✨ | cholesterolcardiology+3 | — | cardiology communityBraunwald and his colleagues+1 | — | cholesterolcardiology+5 | — | 19m 27s | |
| 3/28/26 |  Cholesterol 1: The First Mistake✨ | cholesterolhealth guidelines+3 | — | AHA | — | cholesterolAHA guidelines+3 | — | 20m 33s | |
| 3/20/26 |  Cholesterol and Bloodletting✨ | cholesterolbloodletting+3 | — | New England Journal of Medicine | — | cholesterolbloodletting+5 | — | 27m 04s | |
| 3/13/26 |  A Curious Surgery✨ | rotator cuff surgerymedical trials+3 | — | Health and Human ServicesRT+1 | U.S.Finland | rotator cuffsurgery+5 | — | 19m 12s | |
| 3/6/26 |  Orthopedic Surgery’s Big Problem | I used to do a lot of push-ups. Then, one day, my right shoulder abruptly said no más. Coincidentally, days later I saw my doctor. To be clear, I live by “See doctors, not too much, only when sick,” but my insurance policy insists on an annual visit. So once a year I skulk into the office and prove why doctors make awful patients—particularly when they’re washed-up, windbag, wiseacres who don’t practice medicine.To his credit, however, my doctor is kind and attentive, and quickly noticed my wincing. After a brief shoulder exam he diagnosed a rotator cuff injury and began preparations for an MRI.I demurred. “Oh, that’s alright doc, I’ll just do some PT. But thank you, really.”Gently, and with concern, he offered “It’s important that you be imaged.”“I’m imaged all the time!” I said, pulling out my phone and showing him selfies of me and my boys pretending to throw up.Perhaps it was the cholesterol test (I declined), or the PSA (are you kidding??), or just my winning smile, but this was the final straw. He turned slowly from the phone to me.“Uh-huh. Sure. You do PT.”I concur!RT is 100% reader-supported. To help ensure I can continue, please consider becoming a paid subscriber. The problem, of course, is not my doctor, a man who suffers me with unparalleled grace. It is orthopedics—and a decades-long unmasking.When things work the way they’re supposed to in medicine, the sequence is simple: First, researchers prove a treatment works, then doctors adopt it widely. In many cases, orthopedics has skipped step one.Since the advent of X-rays, orthopedists have used imaging as a crucial, and often primary, determinant of the need for surgery. This has led to miraculous cures for broken and deformed bones. But as imaging advanced well beyond bones, so too did the ambitions of orthopedic surgery. MRIs, CTs, and arthroscopes now detect endless ‘abnormalities’—a frayed meniscus, a bulging disc, a torn ligament, a ruptured tendon.For orthopods, seeing such pictures is a primal call to action: Ug. Thing broken. Me operate.They attack the imperfections by trimming, stitching, shaving, plating, pinning, and reinforcing. But in terms of scientific method, this approach skips step one—the part where trials show surgery helps. Instead, orthopedists have often published a few rosy case reports and voilà—Mikey liked it!—an entire surgical industry was formed.Eventually, curious minds began performing the studies that should have come first. And one by one, some of orthopedics’ most common procedures began to fall.Arthroscopic surgery for meniscus tears—performed hundreds of thousands of times each year—was tested against sham surgery, where patients were anesthetized and the surgeon simply pretended to operate. The real surgery was no better.Arthroscopic ‘cleanup’ of arthritic knees collapsed the same way.Vertebroplasty and kyphoplasty—cement injections meant to stabilize spinal compression fractures—followed the identical arc: widely adopted, then disproven by sham-controlled trials.Even ACL reconstruction, long considered inevitable, now faces trials suggesting rehabilitation alone typically leads to comparable outcomes.Now a study published last month in JAMA Internal Medicine is raising new questions about shoulders. In it, 602 Finnish adults aged forty-one and older underwent MRI scans of their rotator cuffs, the ring of muscles that powers the shoulder joint. About a third had shoulder pain, the rest had no shoulder problems at all.Among those with shoulder complaints, MRI found potentially surgical abnormalities—tears, degeneration, tendinopathy—in 98 percent, a stunning number. But the number for shoulders with no problems dropped jaws even more: 96 percent.Awkward.These results align with sham surgery trials, which overwhelmingly suggest that exercise and physical therapy may often be a wiser, safer approach than the costly, invasive surgeries that millions of Americans still undergo each year.Importantly, none of this means orthopedic surgery isn’t a profoundly important specialty. When bones are shattered, joints are deformed, or trauma disrupts anatomy, surgery can be miraculous. No randomized trial is needed to prove that repairing a fractured femur matters.But those injuries represent only a fraction of modern orthopedic practice.Much of the field now revolves around treating subtle structural abnormalities found on imaging under the assumption that fixing them will help.But assumptions aren’t science—randomized trials are.And once a treatment becomes routine, even if it rests on shaky evidence, it develops its own ecosystem. Training programs teach it. Hospitals invest in the equipment. Surgeons build careers around it. Patients come expecting it.In theory, when a randomized trial shows a procedure doesn’t work, the practice should disappear. In reality, it often doesn’t.Arthroscopic knee surgery continued for years after the sham trials. Meniscus operations still number in the hundreds of thousands annually. Rotator cuff repairs remain a thriving industry. Procedures that randomized evidence has debunked continue to generate billions in revenue and fill operating rooms across the country.Medicine prides itself on being evidence-based. But surgical traditions, once established, can be remarkably resistant to evidence.Why don’t these surgeries work? Probably because the intrinsic healing capacity of the human form has been perfected by a million years of evolution. Modern orthopedic surgery, at about a century, has some catching up to do.In medicine, the order matters: test first, adopt later. Much of orthopedics did it the other way around, and we are still sorting out the consequences. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 12m 22s | ||||||
| 2/19/26 |  How to Spot a Misleading Cancer Screening Study —Before It’s Even Published | Get full access to Research Translation at researchtranslation.substack.com/subscribe | 17m 47s | ||||||
| 2/11/26 | 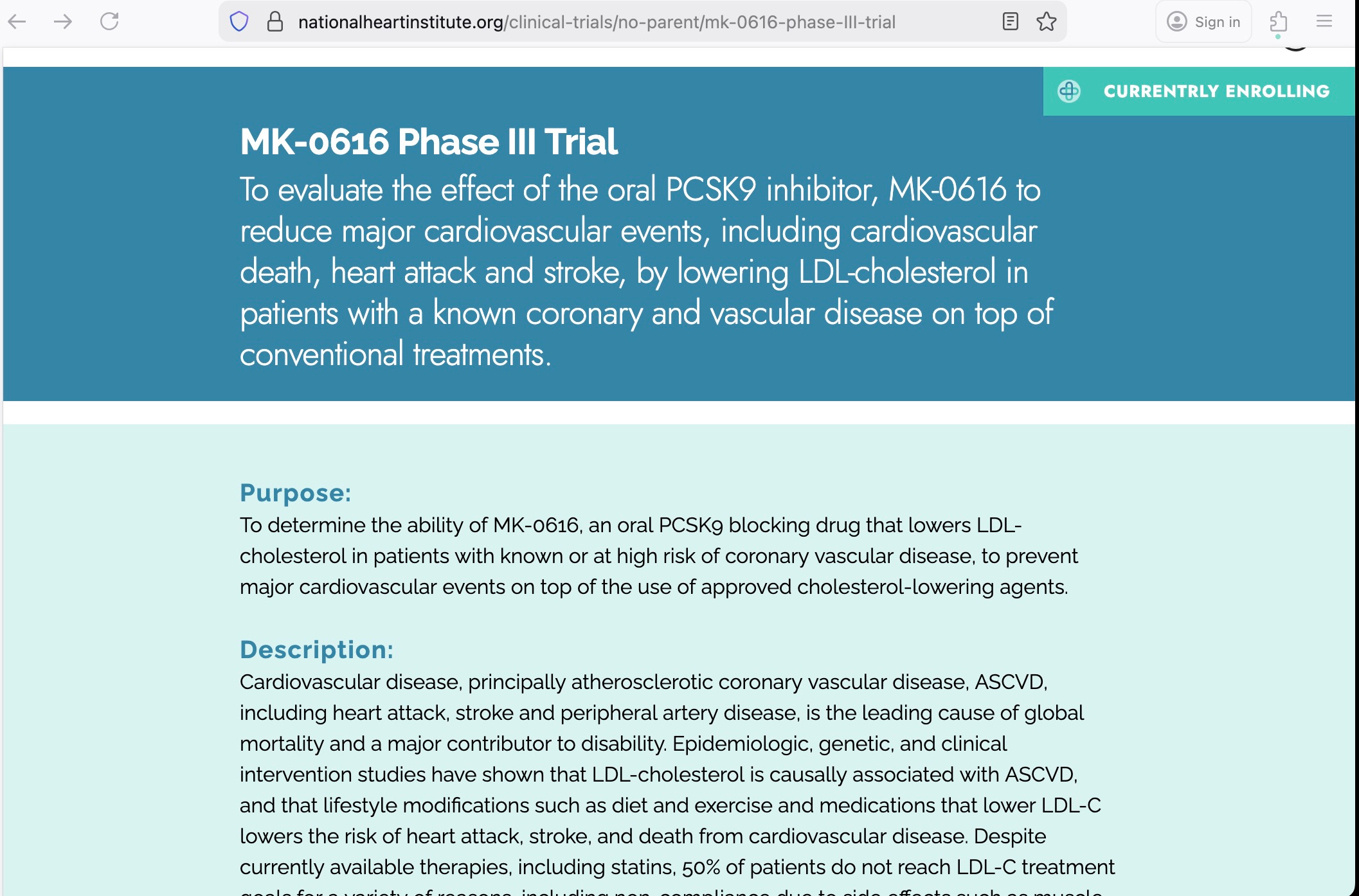 The Case of the Missing Heart Attack | When Arthur Conan Doyle wanted Sherlock Holmes to show off, he didn’t give him a bloody fingerprint or a dropped monocle. He gave him a dog that didn’t bark.In Silver Blaze, the silence was the clue. The horse didn’t vanish because of a stranger—the stable dog knew the intruder. The absence of noise told Holmes everything.That’s where we are with the newest trial of PCSK9s, a class of drug that dramatically lowers cholesterol levels.At first glance, the study looks like a triumph of modern pharmacology. It’s a massive, multinational, double-blinded trial done at hundreds of sites in a dozen countries, enrolling nearly three thousand people. The paper trumpets spectacular reductions in LDL (half or more!) and a power analysis north of 99%. Reviewers nodded. Editors smiled. Headlines followed.And yet: The dog never barked.This drug class exists for one reason: to reduce cardiovascular events—heart attacks, strokes, and deaths. Cholesterol is not the goal, it is the surrogate. Human outcomes are the prize.So where are they?Nowhere in the paper. Nowhere in the abstract. Nowhere in the results. Nowhere, even, in the discussion of limitations. Not a single Kaplan–Meier curve. No exploratory table. Not even the typical cowardly offering—“CV outcomes will be reported separately.” Just, silence.That is not an accident.Holmes would first note the power analysis (a window to the soul of a study): The authors insist the trial was designed to have more than 99% power to prove the drug can lower LDL. But that is absurd on its face. Sniff test: failed. No regulator requires 99% power to prove a biomarker outcome. Eighty percent is standard. Ninety if you’re nervous. But as I’ve pointed out before, increasing power, by upping the number of participants, can be a cover story for ulterior motives.And it’s pricey, to the tune of $50,000 or more per enrollment. Fiscally responsible companies don’t add study participants without a good reason. Which makes it notable that a standard power analysis for this trial suggests the researchers didn’t need to enroll three thousand people—they needed about twenty. Yup. Twenty. For the whole study. Both arms. The PCSK9 drugs drop cholesterol so powerfully that it takes very few participants to demonstrate it mathematically. Which means the company paid more than $140 million for seemingly extra, unnecessary enrollments. So, what’s really happening here?There is a clue that may at first seem small (Dr. Watson once said, "I am glad of all details, whether they seem to you relevant or not"): According to an online recruitment posting for this exact trial, the goal was not to lower cholesterol, but rather “to reduce major cardiovascular events, including cardiovascular death, heart attack and stroke, by lowering LDL-cholesterol.”Ahaa.There it is, in black and white. It takes thousands of subjects to find the tiny reductions in cardiac events that cholesterol lowering drugs can (under the best of conditions for the highest risk people) theoretically achieve. This explains the study’s size. Moreover, in a trial this expensive, CV events were not just possibly collected, they were inevitable. Logged. Coded. Reviewed. Sitting somewhere in a database.Which brings us back to the dog.Why not include the cardiovascular outcomes in the paper? Because they weren’t reduced. If CV outcomes had favored the drug, even weakly, they would have been mentioned or, more likely, headlined. But nary a mention. Not even, “Numerically fewer events, ” or “a favorable trend.” Journals allow that sort of nonsense. Regulators tolerate it. Marketing departments adore it.Instead, nothing. That is not sloppiness, it’s subterfuge.The brilliance of the design is that it allowed them to pivot. By claiming a primary endpoint of LDL reduction (a cakewalk for PCSK9s), and then massively inflating sample size, they could quietly chase their true goal, cardiovascular benefit—while still guaranteeing ‘success’.Heads they win. Tails they don’t lose.The drug succeeded at what was always easy: moving a lab value. But it failed at its secret raison d’être: helping humans.Sherlock Holmes would have closed the file already. The most telling result of this enormous, costly, meticulously planned trial is not what it reported—but what it very carefully did not. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 20m 28s | ||||||
| 1/29/26 |  Selling the Newest Flu Drug: A Masterclass in Distraction | When readers sent me media articles touting baloxavir (‘Xofluza’), I started looking. In the interim, Sensible Medicine, a wonderful Substack by evidence-based doctors, published a podcast, and today a written piece, recommending the drug. I believe they have it deeply wrong. Fun! Check it out, tell me what you think.When I was seven years old I tried hard to see through a frosted glass window. My pediatrician, a silly and smiley man with a nasal voice, stood behind me. “You see that, across the street?” he quacked. Then, leaning forward, as if to sync his line of sight with mine, “See?” His hand was on my shoulder, squeezing gently.I squinted, and tried hard. “Wait… is that it?”“Ah, forget it” he said, smiling at my mother. “You missed it.”Which was true—I’d completely missed the shot in my shoulder. Research Translation is fully reader-supported. Like it? Consider becoming a paid subscriber to help me keep doing it.In addition to being a beloved and brilliant pediatrician, Dr. Gribbetz was a master of distraction. Unfortunately, that’s a skill drug company scientists have also mastered—for different ends—and they played it to perfection with a flu drug called baloxavir.In recent weeks The Atlantic and the Wall Street Journal, noting the rough flu season and weak effects of this year’s vaccine, ran articles extolling the virtues of baloxavir, a single-dose drug hoping to replace 5-day Tamiflu. Both media articles rely heavily on experts who have fallen hard for a 2018 trial published in the New England Journal of Medicine.To be fair, the study also convinced FDA reviewers who approved the drug. Though clearly, that ain’t tough, and the study is a crowded swamp of data. Reading it feels like trying to see through frosted glass. I’ll try to be efficient here, but for the geeks I’ll get into more detail on the podcast.The ‘study’ is actually two separate trials. One compared three doses of baloxavir to a placebo. The other compared baloxavir vs. Tamiflu vs. placebo. Which is remarkable because Tamiflu is a debunked drug, years ago revealed by many independent investigations as not just unhelpful but, to some critics, a premeditated fraud. As I’ve written and podcasted before, Tamiflu trades side effects for flu symptoms, adding as much misery as it subtracts, while failing to prevent serious illness. Meanwhile, symptoms—the only measure either drug even claims to affect—were identical with baloxavir. So the first and most obvious headline should be: BALOXAVIR WAS NO BETTER THAN TAMIFLU, A PROVEN FAILURE. That should end all discussion. But it won’t. The most interesting quirk about the baloxavir paper is that the first trial is an “FDA, Phase 2, dose-finding study”—a fancy way of saying it was done to find a dose, not prove efficacy. The trial had three drug groups of differing doses, plus a placebo group. And no group, when compared to placebo, had enough participants to say whether the drug works. That isn’t a flaw, it’s the point of Phase 2 studies. But it means efficacy claims drawn from them are, by definition, a mistake.Why? Because with three drug groups and one placebo, the drug is getting multiple shots on goal. Efficacy trials get one shot on goal—no more. Ever. And that’s why Phase 2 studies are, well, phase 2. Only Phase 3 studies can say whether a drug works. And in fact, it's weird to publish two studies of different design, from two separate FDA phases, together. It’s weird because the studies have different goals and are interpreted differently. Which is deeply distracting.So what were readers being distracted from? The paper’s much more pivotal Phase 3 study compared baloxavir to Tamiflu and placebo. And here’s where a red flag pops up, bright and tall: Why wasn’t the study a non-inferiority trial comparing the two drugs?‘Non-inferiority’ is a special design statistically and methodologically focused on finding equivalence between drugs. That’s different from a classical superiority trial, designed to find a difference between drugs. For years non-inferiority has been the FDA’s favored design for testing when a new drug claims to be as effective as an older drug. Typically, in such cases the new drug offers some convenience upgrade, like being a pill instead of an injection. Or, perhaps, 1-day versus 5-day dosing. Like baloxavir.Baloxavir is a picture-perfect candidate for a non-inferiority study, but that’s not what the company did. Which means they probably expected more than equivalence with Tamiflu. They expected superiority. When that failed, they settled for (and pretended to celebrate) sameness.How can we know the trial aimed to show baloxavir was better, when the authors claim superiority based on dose-finding, placebos, and virologic results? The Methods section is the paper’s guilty conscience, confessing. The researchers used classical (non-parametric) superiority testing techniques to compare the drugs. Besides this, there is circumstantial evidence. For starters, early lab studies found baloxavir had better effects on viral load and biologic markers than Tamiflu. But that only matters when it translates into people feeling better or being safer, which didn’t happen. This probably surprised and dismayed company researchers, who—like the literati of medical evidence—surely know that Tamiflu is a failed drug. So when baloxavir failed, they changed the narrative: “It’s as good as Tamiflu—yay!” And sadly, most flu ‘experts’ are experts in virology, but not evidence. So when the red flag appeared—a failed superiority trial dressed up as success—they did what seven-year-olds do when asked to see through frosted glass.They squinted, nodded, and missed the shot.Tamiflu is a failed drug. Now we know baloxavir is too. Moreover, both represent a profound risk to public health, because both must be started within two days of first symptoms. If everyone with a sniffle runs immediately to their doctor, or ER, or clinic—resources already dangerously over-burdened—people in dire need of these resources will be harmed. So as I’ve written and podcasted about before, if you want one day’s relief from the flu, try silicon nasal sprays. They’re better, safer, and cheaper, and they’re over-the-counter. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 42m 54s | ||||||
| 1/23/26 |  Autism, Tylenol, and the FDA | Below marks my first critique of politics, and you’ll see why. For background: I have no political affiliation and do not care for party politics. Years ago I became deeply disenchanted with parties of all stripes. I do not seek a packaged bundle of beliefs or positions—I have my own. I care what works, one issue at a time, and I’m open. What I cannot stand, the attribute that repels me most, is the abuse and distortion of truth. On Tuesday the New England Journal of (oddly partisan) Medicine published two opinion pieces on autism—a favored topic of RT! The first addressed Trump and RFKjr’s September press conference on prenatal Tylenol, while the second discussed vague claims by FDA officials implying a chemotherapy drug can now treat autism.To jump into this cesspool of exaggerators and distortionists, we must first acknowledge an uncomfortable but obvious truth: When, on the campaign trail, you promise frenzied crowds that, once in office, you will quickly discover a cause and treatment for autism—a poorly defined neuro-developmental condition that has eluded researchers for decades—you have two options. Fail and concede, or fail and pretend.Guesses, anyone?After months of fishing through a swamp of poorly supported but rhetorically convenient pseudo-theories, RFKjr landed on the one entertained by stoner neuroscience grads munching funyuns at 3am. (Duuude. It’s totally the Tylenol.)I walked through the Tylenol-autism data in October, and last week a review published in a prominent journal confirmed: Put simply, Tylenol has—provably—zero connection to autism. This was self-evident to anyone who actually read the relevant studies.And yet, September 22nd, 2025 the Health Secretary, FDA head, NIH director, and President, acted out an SNL-ready skit, a tragicomedy of performance art. Speaking in the imperious tones of concern for their people, the four most powerful authorities in public health made a claim that wasn’t just weak—it was palpably b******t.The irony is thick. After years of furiously and publicly condemning Anthony Fauci and others for a crisis of public trust, they offered something far more corrosive than technocratic arrogance: A display of knowing dishonesty. This wasn’t confusion or misplaced confidence. It was the deliberate use of scientific authority to launder a claim that everyone involved knew was indefensible.That isn’t a mistake. It’s contempt—for evidence, for the public, and for the idea that science is anything more than a prop.Which is why recent FDA maneuvers around leucovorin, folate autoantibodies, and ‘folate deficiency associated with autism’ cannot be viewed in isolation. They sit in the same epistemic ecosystem. Once again a small, messy batch of weak studies became a nonsense narrative.To be fair, the folate-autism story is not proven nonsense—yet. It is, um, unfinished. Hypotheses deserve testing, not regulatory implication or political theater. The recent Lancet review, like mine months ago, showed what happens when you slow down and let the data breathe (scary headlines evaporate). And I have little doubt the brain-vitamin narrative will dissolve. But there’s work to be done.Bottom line? Autism doesn’t yield to deadlines. It yields to patience, rigor, and a tolerance for ambiguity—three necessary tools for science, ones in desperately short supply right now. When science is forced to perform certainty on command, what it produces isn’t truth—it’s theater.And this is the kind of theater that doesn’t merely fail to rebuild trust, it finishes it off. This administration didn’t set out to heal the public wound of scientific overreach. They inherited that wound and began poking at it deliberately. Trust wasn’t restored, because restoration was never the point. Control was. And a government that treats science as a stage prop shouldn’t be surprised when the audience stops believing anything it says. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 24m 27s | ||||||
| 1/16/26 |  Vitamins, Vaccines, Alcohol, and the Flu—HodgePodge 2026 | This week is an audio hodgepodge—lagniappe, if you will—a chance to discuss and explore recent headlines. Enjoy!Here are some of the relevant RT and news links.WSJ on vitamins-Vitamins piece on RTNYT on recent vaccine changes-Vaccines piece on RT (Covid for children, and related discussion)NY Times on Alcohol and Cancer, Alcohol and cardiovascular disease -Alcohol, alcohol, alcohol, and alcohol pieces on RT (relation to cancer)YLE on antivirals-Tamiflu, antivirals, and other flu treatments on RT (plus Tamiflu’s placebo effect!)RT is 100% reader supported. I’d love to keep doing it. If you agree, consider becoming a paid subscriber Get full access to Research Translation at researchtranslation.substack.com/subscribe | 39m 10s | ||||||
| 1/6/26 |  Aspirin and Donald Trump: Schadenfreude Alert | “Meet Virginia” is, I believe, one of the great rock singles of recent decades. It opens with a blue-sy, core-bending bassline and a thirsty guitar riff, as Pat Monahan etches a fantasy vamp. You will not forget Virginia.“Train” is the band’s eponymous first album, and with other tracks like “Free”, “I Am”, “Egglpant”, and “Rat”, it does not falter. Incredibly, it’s nearly matched by “Drops of Jupiter”, their second album. “She’s on Fire” and “It’s About You” are lyrically brilliant curtains of sound, and the title track is a magical tribute to Monahan’s deceased mother. And yet it’s the deep cut, “Mississippi”, that closes the circle: Train makes albums. Old school, full-package, musical journeys. Not singles. Albums. Which brings me to Donald Trump’s colorful hand, photographed and transmitted around the world this week: RT is 100% reader-supported. To keep it going, consider becoming a paid subscriber.While media outlets fluttered joyously over the president’s mysterious (possibly fatal!) affliction, my first thought was of “Bruises”, a song by Train. In it, Monahan and country singer Ashley Monroe re-connect after years, to find loss and pain have changed them. The chorus digs into a lesson learned by anyone who's been to their high school reunion: “We all got bruises.” Take heart, DJT, you’re not alone.Known in medical lingo as ‘ecchymosis’, bruises are bleeding under the skin. They happen with minor (or major) trauma, but sometimes they pop up spontaneously. As people age, the skin’s superficial vessels become increasingly fragile and bruising more common. Rarely, bruising is the flag for a disease—but rarely. When a man approaching 80 shows up with a hand bruise, it’s usually meaningless.But then we learned that Trump takes daily aspirin—DUN-DUN. And, at a higher dose than normal—DUN-DUN-DUN.There’s lots of data on the pros and cons of daily aspirin, which inhibits platelets and therefore makes blood clotting a bit less efficient. For a quick review (with help from Bill Murray in Meatballs) check out last year’s “It Just Doesn’t Matter.” In it I write (and talk) about how recent trials re-confirmed what I found in 2015 after reviewing the data: For people without known heart disease, daily aspirin is, on balance, more harmful than helpful.But as the NY Times highlights in their finger-wagging explainer about Trump’s aspirin addiction, until 2022 the USPSTF (United States Preventive Services Task Force) was recommending daily aspirin. Why? The USPSTF and I saw the same data, but they’re bad at translating it. Which is sad, since their reviews set standards for insurance (insurance is legally forced to pay for many tests and treatments that are provably worthless because of the USPSTF). But I’ve discussed the task force’s failures, and while I believe there are good, well-intended people there, it was 100% predictable that aspirin would fail in the recent primary prevention trials—because it already had. But I digress.The bigger point here is that aspirin is a wonderful example of a preference-sensitive medicine. That is, people should know the pros and cons—and choose their poison. So here’s the (summarized) deal on daily aspirin for primary prevention:* It does NOT reduce mortality (i.e. it doesn’t prevent death).* It DOES prevent nonfatal heart attacks and strokes, for about 1 in every 250.* It CAUSES bleeding in the brain for 1 in 1,000.* It CAUSES other life-threatening bleeding (mostly gastrointestinal) for 1 in 200.We can turn this into an easy comparison: For every 1,000 who take daily aspirin for primary prevention, 4 avoid a heart attack or stroke, 1 bleeds in their brain, and 5 have a different life-threatening bleeding problem.A few factoids: First, any heart attack or stroke aspirin prevented was likely to be followed by full recovery. Meanwhile, bleeding in the brain is real real bad and typically leads to serious long term disability. Finally, the other bleeding problems mean hospitalization and treatment, but they too are rarely fatal and lead to full recovery.So what does it all mean for our fearless leader, the new President of Venezuela? There’s a better chance Trump will be harmed than helped, and he won’t live longer. BUT HE GETS TO CHOOSE. Perhaps he’s most afraid of a nonfatal heart attack or stroke, and doesn’t mind hand bruises and a 1 in 200 chance of serious bleeding. Though he IS taking a bigger dose of aspirin than in most trials, so his chance of bleeding is even a bit higher.But the worst part for him, it seems to me, is that the press will be waiting for him to bleed, then lapping it up like a parched vampire. They will hover like vultures to bathe in the world’s most public case of bloody schadenfreude. But in reality, as the tiny numbers for aspirin make clear, whether he bleeds or doesn’t, has a stroke or doesn’t, and dies or doesn’t, is far more likely to be determined by his genes, lifestyle, and luck. Which calls to mind another Train song, “Calling All Angels.” Trump should check it out. Get full access to Research Translation at researchtranslation.substack.com/subscribe | 17m 47s | ||||||
| 12/24/25 |  Flu Vaccine and Dog Park Etiquette | I wrote and posted this last year, but with the respiratory season now gripping local and national stats—and me spending time with my family, including two boys with the flu—I thought I’d repost this for anyone interested. Turns out no new flu research has changed anything below. And for a list of prior dives into flu-related studies (including a treatment that works!) see the links at the bottom of the page. Happy Holidays, everyone!My boys found our dog, Jazz, earlier this year. She was eating out of a trash can behind an office building. Collarless and homeless, she was also mangy and thin—but somehow pathologically optimistic. On the car ride home her attitude felt contagious, which led me to record her first ever entry into our house. We went inside, Jazz locked eyes with me and, sporting a winsome grin, shat on the couch. The video plays like a teaser for the horror movie Smile.Jazz’s assimilation into local canine culture has also been rocky. There is, I learned, an unspoken code of behaviors in the dog park. Thankfully she’s not a humper or a poop-eater, traits that can lead to doggy censure. And she’s not a fighter. But she plays rough and, worst of all, looks like a pit bull. Which may be partly because she’s a pit bull.Mostly this hasn’t been a problem. Dogs don’t mind her style of play, but many owners do and recently we had a hiccup. A bougie Pomeranian pranced into the park wearing a harness. I’m not sure why an owner chooses the asylum-style, thoracic harness with a rubber handle on top, but Jazz knew what to do with it.Unfortunately, as Jazz shook her new toy the owner screamed. Like, blood-curdling. I practiced emergency medicine for 25 years in the streets, the ER, and combat support hospitals in Iraq, and I swear to you the following: I’ve never heard anyone make that sound.People ran, men flexed, the dogs were separated. The woman took her pom-pom and left, and there seemed to be broad consensus we should too. Perhaps it was my soft jog as the crisis unfolded. Or the eye roll. In any case, we shame-walked to the gates as breathless owners held their loved ones close.Jazz never wavered, doing her best Marilyn Monroe.Naturally, I’ve been hesitant to go back, despite the fact that Jazz mostly loved her time there, and was loved. It’s probably irrational, but even rare bad moments can have that effect.Which brings me to the seasonal influenza vaccine. Does it work? Should everyone have it? What are the downsides?The flu vax is, to me, a fascinating case study with lots of defensible arguments on all sides. Here are some facts:* The Northern hemisphere vaccine changes each year, built on guesses using flu strains found in the Southern hemisphere where flu season starts earlier* The guesses are pretty good but every five years or so the vaccine uses the wrong strains, like in 2021* Flu vaccine was intended to reduce deaths and serious illness in the elderly, but randomized trials and lots of good observational data suggest it didn’t work; some argue there aren’t enough trials to know for sure* In the late 20th century vaccine uptake rose precipitously—along with flu deaths* In trials, the vaccine consistently reduces getting the flu or a flu-like illness—for kids, healthy adults, elderly people, and even immuno-suppressed adults* The flu vaccine may have reduced serious illness for heart patients at the highest risk (i.e. people with heart failure or known heart disease)Okay so let’s accept some easy and some hard realities. First, the good news: getting vaccinated makes a flu-type illness less likely. That’s a good thing.True, the numbers are small: only about 1 in 30 vaccinated people avoids a flu episode because of the vaccine. But why would anyone not want to reduce their chances of getting the flu?The answer, of course, is because of the downsides. These include effort, and cost, and inconvenience. Most vaccines also involve a needle (for healthy adults there’s now a nasal spray). Also, about 1 in every 125 people experiences a fever because of the vaccine.Finally, there are rare serious reactions. Unfortunately, adverse effects aren’t closely tracked partly because the formula changes yearly, and there aren’t new randomized trials every year. So it’s tough to know how much harm the vaccine might be causing. Studies in past years found the vaccine increased non-flu sicknesses, or (rarely—like 1 in 50,000) may have caused narcolepsy. It was also linked to miscarriages in one study, though the CDC says newer data refute that finding.So… what’s it all mean?For me, there are a few bottom lines. First, the flu vaccine probably isn’t saving anyone’s life. That’s a claim the CDC makes based on zero rigorous data. Therefore the vaccine probably isn’t accomplishing it’s original goal, and that has led some trustworthy experts to suggest marketing and money are behind the yearly push.On the other hand I love the idea it might keep me from getting sick—but only if it’s not going to do anything bad. Is the rare fever, or a super-rare chance of narcolepsy or some other bizarre problem, going to keep me from taking advantage?Not sure yet. But Jazz sure does love playing in the dog park.The RT influenza library:-The new mRNA flu vaccine study—and the one STILL unpublished (both)-A fancy new flu drug, that’s actually not new at all (and doesn’t work) (both)-A not-at-all fancy, or new, flu drug that works (written)-A not-at-all fancy, or new, flu drug (podcast/audio)-Tamiflu (written); Tamiflu (audio)-Sore throats, and mindless medicine (both)-Tamiflu and the double-dog placebo (audio only)- Get full access to Research Translation at researchtranslation.substack.com/subscribe | 21m 06s | ||||||
Showing 25 of 90
Pitch Fit is a Pro feature
See how bookable this show is for guests, which brands already advertise, the per-episode ad value, and the best-fit guest and sponsor profile. The numbers are blurred on the free plan.
How readily this show books outside guests like you.
How proven this show is for host-read sponsorships.
For Guests
ProFor Advertisers
ProUpgrade to Pro to unlock guest cadence, sponsor categories, fit scores, and per-episode ad value for this show.