
Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Most discussed topics
Brands & references
Total monthly reach
Estimated from 2 chart positions in 2 markets.
By chart position
- 🇯🇵JP · Science#9410K to 30K
- 🇵🇭PH · Science#144500 to 3K
- Per-Episode Audience
Est. listeners per new episode within ~30 days
5.3K to 17K🎙 ~2x weekly·125 episodes·Last published yesterday - Monthly Reach
Unique listeners across all episodes (30 days)
11K to 33K🇯🇵91%🇵🇭9% - Active Followers
Loyal subscribers who consistently listen
4.2K to 13K
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
From 13 epsHost
Recent guests
Recent episodes
Friday Reflection 62: The Ethics of Telling Patients We Have Nothing Left to Offer
Jun 26, 2026
4m 57s
This Fortnight in Medicine XXVIII
Jun 17, 2026
32m 16s
This Fortnight in Medicine XXVII
Jun 3, 2026
33m 01s
This Fortnight in Medicine XXVI
May 20, 2026
54m 35s
This Fortnight in Medicine XXV
May 6, 2026
30m 20s
Social Links & Contact
Official channels & resources
Official Website
Login
RSS Feed
Login
| Date | Episode | Topics | Guests | Brands | Places | Keywords | Sponsor | Length | |
|---|---|---|---|---|---|---|---|---|---|
| 6/26/26 |  Friday Reflection 62: The Ethics of Telling Patients We Have Nothing Left to Offer | TR is an 88-year-old man who is disabled and in chronic pain from spinal stenosis and knee osteoarthritis. He has multiple other medical issues, including coronary artery disease and COPD.He has been through years of treatment for his knees and back, including physical therapy, multiple joint injections, and an in-office procedure for spinal stenosis. He has been on multiple regimens of oral pain medications. He is not interested in surgery (and probably would not be considered a reasonable candidate if he were).He comes to a visit and asks what can be done.Sensible Medicine is a reader-supported Substack. If you appreciate our work, consider becoming a free or paid subscriber.We are taught never to say, “There is nothing I can do for you.” We may be out of surgical or medical options, but we can always continue to care for and support our patients. This is not part of the Hippocratic Oath, but it is so integral to our training that one might think it belongs there.There are good reasons to caution doctors from saying some version of, “I am sorry, I don’t think there is anything more I can do for you.” It is true that in 21st-century medicine, the act of caring for patients has been so trivialized that we need to remind ourselves that caring is not just a last resort but our first responsibility.Hope in the face of illness is exceedingly valuable. Robbing this hope is not only cruel, but probably bad for the health of patients.Then there is the truth that when one doctor has nothing left to offer, medicine often still has more to offer. I am still haunted by at least one case when I mistook my lack of knowledge for a shortcoming in the field.A doctor saying he has nothing left to offer may be taking the easy way out. Further research or a considered referral often suggests effective treatments, if not cures. There is always a risk that when we say, “We can’t help,” we are wrong.All this being true, I don’t think we admit that there is nothing left to be done often enough. The Modern Hippocratic Oath does include the line:I will not be ashamed to say “I know not”, nor will I fail to call in my colleagues when the skills of another are needed for a patient’s recovery.Is it that much of a stretch to imagine the oath saying:I will not be ashamed to say “I have nothing left to offer beyond my ongoing care and commitment”, nor will I call in my colleagues, knowing they have nothing to offer beyond protecting me from admitting medicine’s limitations.We no longer conceal bad diagnoses from patients; we consider this unethical. It is time that we consider it unethical to conceal that we have nothing to offer beyond palliation.It is hard to tell patients that the best we can do is control pain, especially when we have been trained not to. It takes work to be sure that neither you nor your colleagues have something to offer beyond a hamster wheel of care to provide hope but nothing more. It also takes some guts; we can never be 100% sure that nobody has anything to offer.Yet there are downsides to never saying we are done. Many patients accept that further care is futile, not after an honest conversation, but after being worn down by my endless visits, treatments, and promises that lead nowhere. All the while, time and money are wasted; time and money that could be better spent on life. The useless medical care leaves patients and their families increasingly frustrated by a medical system that refuses to be honest and caring.There are patients who welcome an honest assessment of their options and shift their focus to living with their disease and disability. There are also patients who do not. I’ve had patients fire me for saying there was nothing to do. They left me to get on that hamster wheel of care. This decision did not make them better, but maybe it made them happier and more ready to accept the inevitable. Eventually.TR calls now and then and comes to see me every three or four months. He tells me about his symptoms and the things he wishes he could do. I tell him there are things he could try and people he could see, but I let him know I don’t think any of these options would be productive. He tells me he’s not interested. I advise him to push up on his pain medications and to pretreat his symptoms; I know he will not take this advice. I know we will repeat this visit in the future; I actually hope we will, for years. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 4m 57s | ||||||
| 6/17/26 |  This Fortnight in Medicine XXVIII | Amoxicillin-Clavulanate vs Amoxicillin for Acute Sinusitis in Adults* Prespecified Falsification End Points: Can They Validate True Observational Associations?* Ultrasonography versus Computed Tomography for Suspected NephrolithiasisGLP-1 receptor agonist use and cancer risk in obese nondiabetic adults* Risk for Cancer With Glucagon-Like Peptide-1 Receptor Agonists and Dual Agonists: A Systematic Review and Meta-analysis This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 32m 16s | ||||||
| 6/3/26 |  This Fortnight in Medicine XXVII✨ | sunscreen usemelanoma+5 | — | GLP-1 Receptor AgonistsSGLT2 Inhibitors+4 | — | melanomasunscreen+5 | — | 33m 01s | |
| 5/20/26 |  This Fortnight in Medicine XXVI✨ | Atrial FibrillationLeft Atrial Appendage Closure+3 | — | Left Atrial Appendage ClosureAnticoagulation+2 | — | Atrial FibrillationLeft Atrial Appendage Closure+3 | — | 54m 35s | |
| 5/6/26 |  This Fortnight in Medicine XXV✨ | COVID-19 treatmenthypertension therapy+3 | — | Nirmatrelvir–RitonavirThree Low-Dose Antihypertensive Agents in a Single Pill after Intracerebral Hemorrhage+1 | Taiwan | NirmatrelvirRitonavir+6 | — | 30m 20s | |
| 4/22/26 | 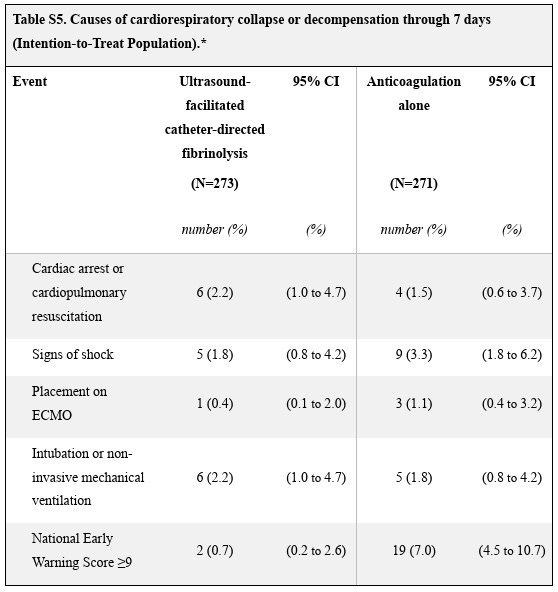 This Fortnight in Medicine XXIV✨ | RSV VaccinePulmonary Embolism+3 | — | RSV Prefusion F VaccineUltrasound-Facilitated, Catheter-Directed Fibrinolysis | — | RSVVaccine+4 | — | 46m 16s | |
| 4/8/26 | 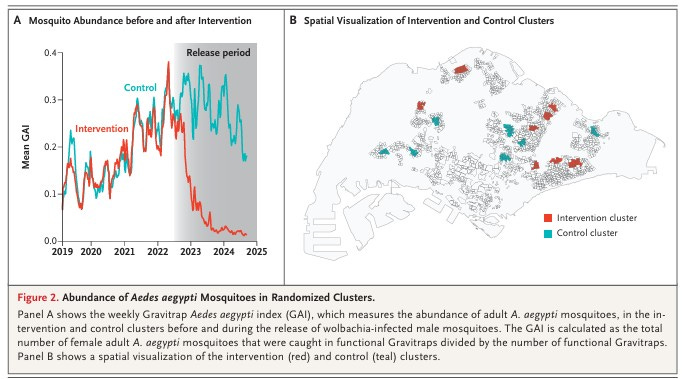 This Fortnight in Medicine XXIII✨ | Dengue suppressionWolbachia-infected mosquitoes+3 | — | World Mosquito Program | — | DengueWolbachia+4 | — | 33m 34s | |
| 3/24/26 | 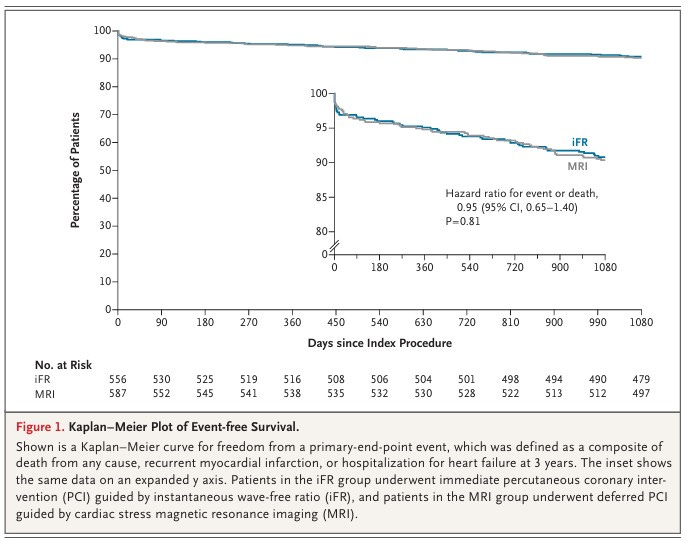 This Fortnight in Medicine XXII✨ | glucagon-like peptide-1 receptor agonistssubstance use disorders+4 | — | US veteransSensible Medicine+1 | — | glucagon-like peptide-1substance use disorders+5 | — | 39m 33s | |
| 3/11/26 | 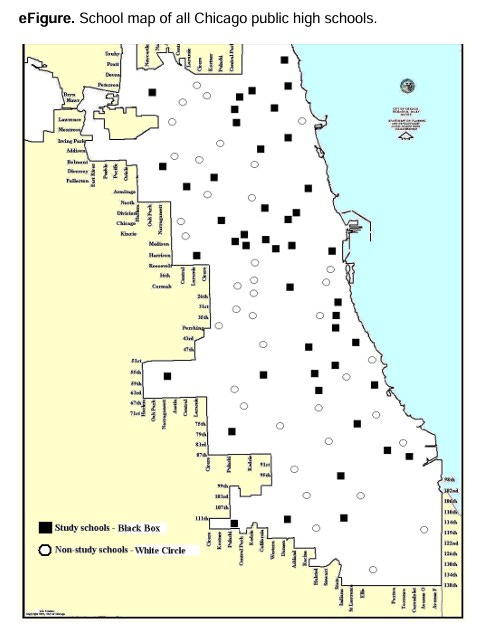 This Fortnight in Medicine XXI✨ | HyponatremiaInjury Prevention+3 | — | Sensible MedicineUrban Public High Schools | — | HyponatremiaACL Injury+3 | — | 35m 50s | |
| 3/4/26 |  Going Beyond "AI in Medicine"✨ | AI in medicineinnovation+3 | Dr. Shantanu Nundy | FDA | — | AImedicine+5 | — | 24m 11s | |
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 2/25/26 |  This Fortnight in Medicine XX✨ | influenza vaccine effectivenesshospitalization reduction+3 | — | High-Dose Influenza Vaccinestandard-dose influenza vaccine+1 | Older Adults | influenza vaccinehigh-dose vaccine+5 | — | 39m 08s | |
| 2/18/26 |  Alternative Modalities for Breast Cancer Screening✨ | breast cancer screeningdense breasts+3 | Dr. Jennifer Rusiecki | University of Chicago | — | breast cancerscreening+5 | — | 36m 54s | |
| 2/11/26 |  This Fortnight in Medicine XIX✨ | dialysis strategykidney function recovery+2 | — | LIBERATE-DSensible Medicine | — | dialysisacute kidney injury+3 | — | 44m 45s | |
| 1/28/26 |  This Fortnight in Medicine XVIII✨ | medicinehealth articles+1 | — | — | — | medicinehealth+3 | — | 45m 36s | |
| 1/23/26 |  Friday Reflection 56: Comments that Stuck✨ | medical practicementorship+3 | — | — | — | medical practicementorship+3 | — | 7m 27s | |
| 1/18/26 |  When to treat (or not treat) a high cholesterol | I was shocked at the comments on this post. Many people, some of them I know to be smart, thought I was nuts for suggesting two middle-aged women who had isolated high LDL-C needn’t take meds because their calculated 10-year risk was less than 3% What shocked me is that our guidelines suggest treatment with statins when 10-year risk is ≥ 7.5%. You may not know this but clinicians are supposed to consider cholesterol (and BP) based on overall risk, which include things like age, blood pressure, smoking status as well as HDL. Here is a link to the PCE. It drives me bananas that clinicians don’t go over this with patients. They just look at LDL-c in isolation. Content like this comes free of industry support. Please consider becoming a free or paid subscriber.Experts chose this a 7.5% threshold because they felt it was the point where the absolute risk reduction from statins (about 20-25% relative risk reduction) for nonfatal cardiac events outweighed any potential downsides of statins. It is an arbitrary threshold. The thinking: We know from many RCTs that statins reduce future risk by about 20-25% over 5 years. So .25 x the estimated risk outputs the absolute risk reduction. Let’s say a person has a calculated risk of 10%. They can expect a 2.5% risk reduction (.25 x 10% = 2.5%) over 10 years. But .25 x 3% = .75, so a person with an estimated risk of 3% who takes a daily pill for 10 years goes to 2.25%. That’s not much. Here are some pics of the pushback I recieved:My colleagues rightly point out that atherosclerosis of the coronary arteries is a slow process and longer exposure to lower LDL-c is beneficial. They feel that the 10-year horizon is too short. They cite something called Mendelian randomization studies which find that people who were born with genetic profiles that cause low cholesterol also have low rates of heart attacks. I wrote a post about this. I actually think that statins and blood pressure drugs may have greater effects in younger people who are at lower risk. But come on. Both individuals who I helped calculate risk were below 3%. That’s too low to worry about. Further, if you think we treat people with elevated LDL levels who have this low of a risk, why do we need risk calculators? Or…why don’t we just treat everyone above a certain age, since age is the largest driver in the calculators? These are issues I spoke with Drs Foy and Murthy about. I learned a ton. I hope you will too. Topics include:* The value of risk calculators* The uncertainty of prediction* The best time window to consider (statin trials were for 5 years; can we assume effect sizes over 5 years are similar at 30 years?) * The causal role of LDL-c vs “metabolic health”* The value of coronary artery calcium testing * Lipoprotein (a) Academic people like to make fun of podcasts, but I can’t imagine a more educational 40 minutes. Andrew and Venk are two of the most thoughtful people in cardiology today. Enjoy and consider supporting Sensible Medicine This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 39m 51s | ||||||
| 1/14/26 | 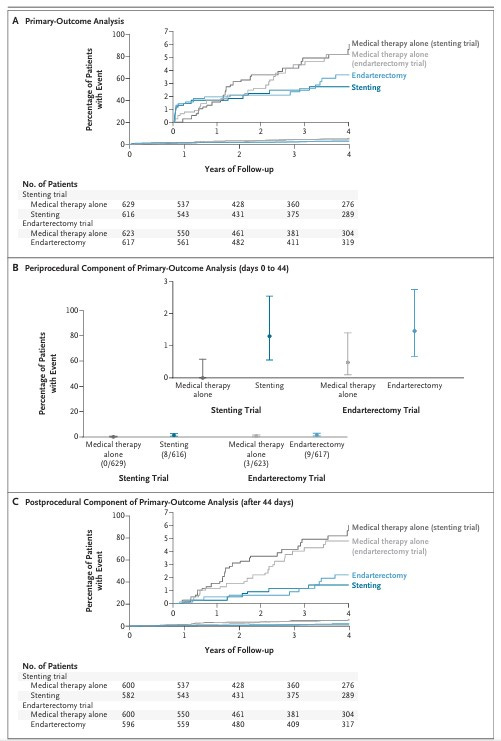 This Fortnight in Medicine XVII | Medical Management and Revascularization for Asymptomatic Carotid StenosisVagus nerve-mediated neuroimmune modulation for rheumatoid arthritis: a pivotal randomized controlled trialWe spent quite a bit of time talking about blinding. This is the table on the adequacy of blinding from the supplement. It does seem like blinding was less than perfect. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 45m 04s | ||||||
| 12/31/25 |  This Fortnight in Medicine XVI | We try to answer the remainder of your AUA questions. We will be back in the new year with more article discussions!Here are a few of the things we referenced.GDMT Bugs Me: A bit of a rant against the standard of careA Plan to Refocus Primary CareSacrificing patient care for prevention: distortion of the role of general practiceThe Great Colonoscopy DebateArthroscopic Partial Meniscectomy versus Sham Surgery for a Degenerative Meniscal Tear This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 1h 22m 35s | ||||||
| 12/17/25 |  This Fortnight in Medicine XV | We cover questions from Amy J, Benjamin Hourani, Diana Stiles Friou, Chris Costas, Errol Laurie, Jim Healthy, Elizabeth Fama, Never Dull, Rod Rodriguez, Ellison Burns, David Araujo, and George.We have more to come!One nice reference I found while looking into some of the topics:DMSO Is Not a Cure-All. But the FDA’s Panic Over It Birthed a Myth This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 1h 00m 40s | ||||||
| 12/3/25 |  This Fortnight in Medicine XIV | Vascular and inflammatory diseases after COVID-19 infection and vaccination in children and young people in England: a retrospective, population-based cohort study using linked electronic health recordsComparison of an Initial Risk-Based Testing Strategy vs Usual Testing in Stable Symptomatic Patients With Suspected Coronary Artery Disease: The PRECISE Randomized Clinical Trial This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 33m 51s | ||||||
| 11/19/25 | 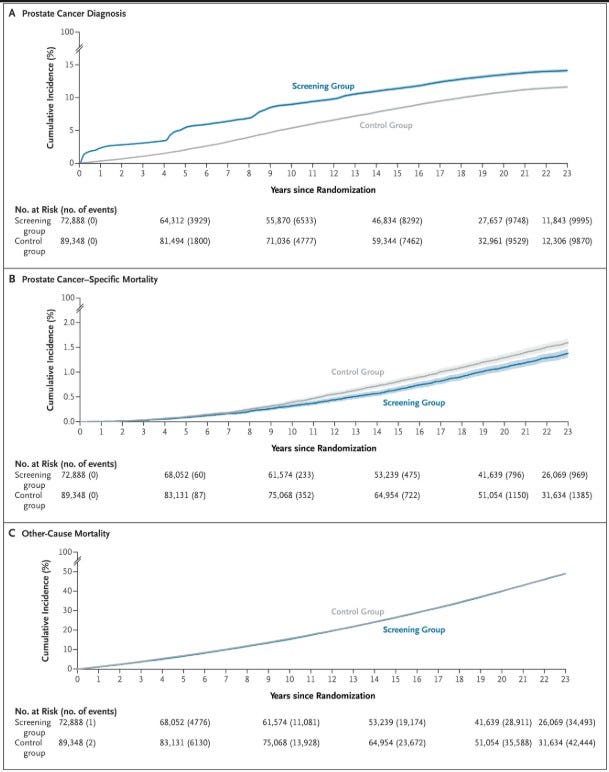 This Fortnight in Medicine XIII | European Study of Prostate Cancer Screening — 23-Year Follow-upAssociation Between Baseline Diastolic Blood Pressure and the Efficacy of Intensive vs Standard Blood Pressure–Lowering TherapyFurther Reading* Effects of intensive blood-pressure control in type 2 diabetes mellitus* A Randomized Trial of Intensive versus Standard Blood-Pressure ControlSensible Medicine is 100% reader-supported. If you appreciate our work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 44m 10s | ||||||
| 11/5/25 |  This Fortnight in Medicine XII | Effects of Intensive Blood Pressure Control in Patients With Frailty: A Post Hoc Analysis From ESPRIT* Lowering systolic blood pressure to less than 120 mm Hg versus less than 140 mm Hg in patients with high cardiovascular risk with and without diabetes or previous stroke: an open-label, blinded-outcome, randomised trial* Reduction of Antihypertensive Treatment in Nursing Home ResidentsPolysaccharide Conjugate Vaccine against Pneumococcal Pneumonia in Adults* A trial to evaluate the safety and immunogenicity of a 20-valent pneumococcal conjugate vaccine in populations of adults ≥65 years of age with different prior pneumococcal vaccination This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 40m 53s | ||||||
| 10/22/25 |  This Fortnight in Medicine XI | Total cholesterol and all-cause mortality by sex and age: a prospective cohort study among 12.8 million adults* The Ideal Cholesterol Level ... Depends...And Cannot Be Determined From Observational StudiesStructured vs Self-Guided Multidomain Lifestyle Interventions for Global Cognitive Function: The US POINTER Randomized Clinical Trial* Can We Please Stop Asking if Crossword Puzzles Prevent Dementia? This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 51m 13s | ||||||
| 10/8/25 |  This Fortnight in Medicine X | Two papers this week, with a bunch of articles that we referenced in the conversation. Also, the last Fortnight podcast was accidentally posted behind a paywall. It is now up and free to listen to. My apologies. Sensible Medicine is reader-supported. If you appreciate our work, consider becoming a free or paid subscriber.Folinic acid improves verbal communication in children with autism and language impairment: a randomized double-blind placebo-controlled trial* Folate Receptor Alpha Autoantibodies in Autism Spectrum Disorders: Diagnosis, Treatment and Prevention* Association Between Maternal Use of Folic Acid Supplements and Risk of Autism Spectrum Disorders in Children* Cerebral folate receptor autoantibodies in autism spectrum disorder* What Is Leucovorin, the Medicine Being Approved for Autism Treatment?* Clinicaltrial.gov searchEffects of Glucagon-Like Peptide 1 Receptor Agonist Initiation in Patients With Heart Failure With Reduced Ejection Fraction and Implantable Cardiac Devices* Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes* Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes* Effects of Liraglutide on Clinical Stability Among Patients With Advanced Heart Failure and Reduced Ejection Fraction* Increased Risk of Heart Failure Hospitalization With GLP-1 Receptor Agonists in Patients With Reduced Ejection Fraction: A Meta-Analysis of the EXSCEL and FIGHT Trials This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 50m 52s | ||||||
| 9/24/25 |  This Fortnight in Medicine IX | We go all observational this week. A look at data suggesting the safety of GLP-1s and a re-examination of data on patient/doctor race concordance/discordance (a topic Adam said we should not study, and then John forces him to).GLP-1 Receptor Agonists and Cancer Risk in Adults With ObesityPhysician–patient racial concordance and newborn mortalityOriginal, 2020 article: Physician–patient racial concordance and disparities in birthing mortality for newborns This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit www.sensible-med.com/subscribe | 34m 11s | ||||||
Showing 25 of 131
Pitch Fit is a Pro feature
See how bookable this show is for guests, which brands already advertise, the per-episode ad value, and the best-fit guest and sponsor profile. The numbers are blurred on the free plan.
How readily this show books outside guests like you.
How proven this show is for host-read sponsorships.
For Guests
ProFor Advertisers
ProUpgrade to Pro to unlock guest cadence, sponsor categories, fit scores, and per-episode ad value for this show.
Chart Positions
2 placements across 2 markets.
Chart Positions
2 placements across 2 markets.