
Insights from recent episode analysis
Audience Interest
Podcast Focus
Publishing Consistency
Platform Reach
Insights are generated by CastFox AI using publicly available data, episode content, and proprietary models.
Most discussed topics
Brands & references
Total monthly reach
Estimated from 1 chart position in 1 market.
By chart position
- 🇭🇰HK · Mental Health#5010K to 30K
- Per-Episode Audience
Est. listeners per new episode within ~30 days
5K to 15K🎙 Weekly cadence·101 episodes·Last published 1mo ago - Monthly Reach
Unique listeners across all episodes (30 days)
10K to 30K🇭🇰100% - Active Followers
Loyal subscribers who consistently listen
4K to 12K
Market Insights
Platform Distribution
Reach across major podcast platforms, updated hourly
Total Followers
—
Total Plays
—
Total Reviews
—
* Data sourced directly from platform APIs and aggregated hourly across all major podcast directories.
On the show
From 1 epsHost
Recent guests
Recent episodes
Getting our heads around the manosphere: two health professionals react
Apr 30, 2026
57m 06s
Introducing Brain Medicine
Apr 17, 2026
6m 28s
How To Ruin Your Relationships
Dec 17, 2025
36m 56s
Brain Stimulation (TMS) as a Treatment for Auditory Hallucinations
Nov 19, 2025
47m 40s
A Breakthrough in Violence Prevention, by Treating Violent Criminals with MBT Therapy
Sep 18, 2025
16m 19s
Social Links & Contact
Official channels & resources
Official Website
Login
RSS Feed
Login
| Date | Episode | Topics | Guests | Brands | Places | Keywords | Sponsor | Length | |
|---|---|---|---|---|---|---|---|---|---|
| 4/30/26 |  Getting our heads around the manosphere: two health professionals react✨ | manospheresocial media+4 | Jeremy | ClubhouseSubstack Live+1 | — | manospheresocial media+6 | — | 57m 06s | |
| 4/17/26 |  Introducing Brain Medicine | Hi. I haven’t done a podcast in too long, so here is one!I’m introducing Brain Medicine. I’ve written about its ascendancy in the news this week.For those who’d like to read something today, I suggest this article about understanding Narcissistic Personality Disorder, in Prevention magazine, also published this week.For those about to listen to a quick podcast to start out their run, I offer the above. Also, I went to a flower show:Something for everyone!Advertising Moments: Inessential PharmacologyI have a new, PHYSICAL, IN-PRINT book available for purchase. Inessential Pharmacology is available from Amazon (affiliate link), in both hardback and paperback. Kindle ebook version is also available.RAMHT 2026 SF is coming up on May 16th, 2026!Get a ticket now—also, it’s free if you’re an APA (the psychiatric one) member. Just email us at ramhtevents@gmail.com for your free code. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 6m 28s | ||||||
| 12/17/25 |  How To Ruin Your Relationships | One of the things I like about being on the Internet is that I get to meet the actual humans! There are people I've had real relationships with over many years, and some of them I've just never gotten to see in person yet. Making content on the Internet helps connect you to other people making content on the Internet, and if you're good at making friends, sometimes you can make a new friend. One such friend is featured in this podcast, and it's Annalisa Hanson—she is a therapist, who made some great content on TikTok, and then we hopped on the phone because we were such mutual fans, and then she joined me here on the podcast. Another guest on this episode is Dr. Mason Hargrave, we are also Clubhouse, and then he invited me to record a podcast in what was his apartment at the time. It's a classic.Today’s conversation grew out of a phone call with Annalisa and subsequent calls with Brandon In, Mason, Ahmed Tahseen, and my daughter Quinn.We “delve” into AI chatbots as a source of relationship advice. It’s quite the cautionary tale.The music is by Owen Muir, with some tunes a gift from my friend John Vanderslice. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 36m 56s | ||||||
| 11/19/25 |  Brain Stimulation (TMS) as a Treatment for Auditory Hallucinations | Schizophrenia is a really challenging illness. There's been a lot of progress made recently, I will note. I've already written about novel treatments like Cobenfy, and using accelerated transcranial magnetic stimulation for negative symptoms and positive symptoms in schizophrenia. One of the most bothersome of those “positive symptoms”—things that shouldn't be there, in someone's mind, but are—are auditory hallucinations. If you imagine having invisible AirPods that are playing a terrible podcast that you'd rather not be listening to, and that everyone else can't hear, you get a sense of how distracting it might be to have auditory hallucinations.In my previous article about the treatment of auditory hallucinations with transcranial magnetic stimulation (TMS), one of my favorite forms of brain stimulation, I highlighted promising results from early studies. Now we have a much larger Study, phase 3 trial, conducted over many years in Germany. We are even at the level of meta-analysis at this point!It’s a considerable study:138 adults with treatment-persistent auditory verbal hallucinations and schizophrenia spectrum disorder were randomly assigned (1:1) to receive 15 sessions of active (n=70) or sham cTBS (n=68) administered sequentially as 600 pulses to the left and 600 pulses to the right temporo-parietal cortex over a 3-week period.I called friends of the podcast—Dr. David Garrison, Dr. Will Sauve, and my mom, Vita Muir, to talk through this paper together, and what it might mean for individuals suffering from psychotic disorders. In the meantime, the team at Radial, where we provide such treatment, does some funny, tough-guy faces with our Ampa One system:Thanks for reading! A live-action newsletter event coming up on January 11th in San Francisco: RAMHT 2026 SF. Join us! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 47m 40s | ||||||
| 9/18/25 |  A Breakthrough in Violence Prevention, by Treating Violent Criminals with MBT Therapy | I wrote an article about this research before, available here. However, I also made a podcast for my audience about the topic! Antisocial Personality Disorder is usually considered untreatable. A new study from the Anna Freud Centre’s MBT program demonstrates a remarkably effective treatment.At Radial, this is the modality of therapy we specialize in providing. It is also effective in borderline personality disorder and in suicidal adolescents. However, with some riffs, it turns out, it also helps ASPD. I even wrote a book on this a while back, published by Springer Nature (Amazon affiliate link).This conversation features my mom, Lila , and David Carreon, M.D..If you enjoy it, please share it with others! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 16m 19s | ||||||
| 8/3/25 |  How I Wrote 966 Articles and 98 Podcasts in Three Years | This is the podcast version of yesterday’s article. Yes, I Know It Has A Different Title.Thanks for listening.And if you are looking for care for yourself or a loved one…join us at Radial—where I work—we focus on next-generation treatments.They include Spravato, Nightware, eTNS, PRISM Neurofeedback, soon, eCOT-AS by Neurolief, TMS, Accelerated TMS, and fMRI-guided SAINT TMS.Radial offers the most advanced mental health care, anywhere. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 14m 44s | ||||||
| 6/22/25 |  How Can We Treat Bipolar Disorder in the Global South? | I was invited, thanks to the magnificent and only-ever-positive internet, to give a lecture to colleagues in Nigeria. I’m kidding, a little—the internet can be rough. Ask a comment section of a YouTube video! However, it is also a technology that has brought the world closer together. One of those less absurd corners of the internet is LinkedIn—it’s like the world’s most boring dad and his boss decided to invite you to a global-scale compliance educational module. “So exciting, it’s mandatory!”I am giving the internet a hard time. Sometimes it’s a special kind of magic. Like, for example, today. Imagine you are a progressive hospital system in Lagos, such as Gracehill Hospital. Yes, that is in Nigeria. It’s a progressive country, compared to the rest of the continent, but some of that progress is recent, as in 2023.A new Mental Health law was recently enacted in Nigeria to replace the Lunacy Ordinance of 1958. The passage of the new law was a major leap from the old. It was received with excitement because the former law was not only outdated but failed to address core issues such as the promotion of mental health and the protection of the rights of the mentally ill.If you're looking to move your healthcare system into the future, you might want to consider finding speakers for your grand rounds. With Zoom, it’s easy to host hundreds of people. On LinkedIn, you can see professionals posting about what they are up to. And, if you're bold, you can simply ask one of those folks to speak. Which is what happened to me, and how I found myself drafting a lecture on Bipolar Disorder for an audience of Nigerian (and global—many people, both professionals, patients, and family members attend these seminars!).Nigeria has an estimated 250 practicing psychiatrists for a population of over 220 million (WHO, 2023), amounting to roughly one psychiatrist per 880,000 people. I probably spoke to 1/4 of them yesterday.There are substantial barriers to mental health care in Nigeria—much if it financial. According to the World Bank, Nigeria’s Gross National Income (GNI) per capita in 2023 was $2,460 USD. Fewer than 10% of Nigerians have health insurance. Those plans cost $250+ a year, but mental health parity doesn’t exist, and thus those services are only covered under yet more expensive plans.To draw a direct comparison, Nigeria has 0.11 psychiatrists /100,000 population. This is similar to Kenya (0.2/100,000) but with 400% more money budgeted to address the care of the population. The US has 13/100,000 and spends about 6.2% of its health budget on mental health care.The question, globally, is how to do more for our patients with less harm and at lower cost. One interventional treatment is considered essential—and its ECT. The WHO's keep an “essential medicines” list! Nigeria has access to ECT. Lithium is also an essential medicine. TMS is not on that list, yet. Maybe, I posit, it should be?What follows in this podcast is the talk I gave. Thanks for reading— and listening. A huge shout out to my gracious hosts at GraceHill, and their Partners, who make this series possible!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.If you are interested in the Validation Institute’s award for Best Mental Health Treatment in 2024, consider Radial. It’s where I work, and with locations across the US already, we are working to bring the most advanced mental health care to everyone and make it accessible. If you are looking for help, Radial offers the most advanced mental health care. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 29m 34s | ||||||
| 6/20/25 |  Ketamine in the Land of Taylor Swift | One of my great joys as a psychiatrist is the ability to collaborate with excellent colleagues. Irfan Handoo, M.D., of Kansas City Psychiatric Partners, is one such human. In this interview, we learn about how Dr. Handoo went from psychopharmacologist to interventional psychiatrist, why Kansas City is the best city in the world, and why being South Asian is the ultimate hack to get your patients the best care. It's really easy to think of doctors being completely burned out, and not caring about their patients. Being a physician is a tremendously challenging thing to do with one’s time, and many doctors have their compassion wear thin. This interview with Dr Handoo reminded me how much some of us care, all day, every day. He's an inspiration to me, and I hope, to my listeners also.I am delighted to bring you this interview! Prior articles featuring the work of Dr. Handoo include:Thanks for reading and listening!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 1h 05m 48s | ||||||
| 5/29/25 |  Suicide Among Resident Physicians | Every once in a while, science authors will crank out a paper that answers some questions, but asks so many more. I’ve been talking, writing, and podcasting about physician suicide longer than most other topics in my creative life.I did a whole award-winning series as a Rudin Master Scholar in Ethics and Humanities, which no one noticed. Including podcasts like these:and this…and this…Today’s podcast is instead of a written column. Feel free to listen. The paper it’s about is here:Causes of Death Among US Medical ResidentsIt was published on May 14, 2025. Please read it, listen to the podcast, and share with your world. It’s a challenging path, that of physicians, and we should consider making it less miserable, for all our sakes. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 24m 42s | ||||||
| 5/26/25 |  Say His Name: Five Years Since Mr. George Floyd | Author’s Note: This writing was adapted from a series of conversations around race in America and edited as audio, recorded in 2020, right after George Floyd was lynched.. The podcast of this writing is the real thing, as it were. What follows is edited text to clarify the narrators, absent the audio. Please consider following the podcast associated with this newsletter and leaving a 5-star review on Spotify or Apple Podcasts. Please subscribe to support high-impact content like this.The author, David Foster Wallace, described the experience of reading his novel Infinite Jest as intended to feel “tornadic,” like you're in the middle of a tornado. That's what the last several weeks have felt like.Protesters:"Racist ass police! No justice, no peace! F**k these racist ass police! No justice, no peace!""F**k these racist ass police!"Owen Muir, M.D.:I originally tried making this episode a linear narrative, but it wasn't happening. So, welcome to the tornado of racism in America. Buckle up.George Floyd spent 8 minutes and 46 seconds gasping for breath. Police officers, some of whom were very experienced, knelt on his back...until he didn't breathe anymore. As a psychiatrist, I often emphasize how the words we use to describe someone's death have meaning. So, I'll say, you know, completed suicide, not “commit.” And George Floyd was lynched.Welcome. This is about anxiety, uncertainty, and existential despair. And I recorded the narration in one take because I wasn't, like, going to get it right a second time. So much of what we say about race is calculated, polite, and wrong. So I'm not going to try to do that tonight.Here we go.Sequoiah:"Yeah. My general reaction to all this is a little more, a little more extended. The, uh, f**k".Owen Muir, M.D.:That's my teammate. She is a TMS technician at the mental health practice we worked at together. She also works in the community with patients helping put their lives together, but tonight she's a field reporter on the revolution.Sequoiah:"I am a TMS tech, Winnicott coach, and black woman. Which seems very important right now. George Floyd, Say His Name. George Floyd, Say his Name.So I just got home from a protest in Flatbush. Police would not let us pass. We were chanting with our hands up. And after a while, they decided to push the line backward. We resisted—we stood there with our hands up. They pushed us and pushed us, and when we wouldn't..."Owen:Now, as someone with a lot of white privilege, I'm outraged at hearing this, like, wow, this is fucked up. So I called another colleague in the special operations community, and I'm not using names in this episode for semi-obvious reasons, and I heard what he had to say.Master Sergeant:“The things that U. S. police forces are apparently fully within their legal rights to do, like, use tear gas, would literally have…been against the Geneva Conventions. It's an actual war crime. We cannot gas a civilian population.”Owen Muir, M.D.:The person I’m interviewing has over a decade of experience in the special operations community. He has fought and killed for our right to do what my other colleagues were in the street doing, peacefully protesting.Master Sergeant:"This is a perversion of what the United States stands for. We invade countries who treat their people the way that our police forces are on camera treating Americans "Sequoiah:"People started to back up, , and run and they then started to hit us with batons. , I fell. And then we reformed the line."Master Sergeant:"It's disgusting in a lot of ways."Owen Muir, M.D.:So when someone whose life has been dedicated to protecting our freedoms tells me they're upset with what they're seeing, I take that pretty seriously.Sequoiah:"Well, the other night, well, last night, when the cops and protestors were getting into, into fights and they were trying to, the cops were trying to push back the protestors, I saw them bring out the batons and, like, start attacking people...and each time they'd tell us to back up and back up and kept pushing us and pushing us. And finally, there was a frustration in the air, and people started to act out."Owen Muir, M.D.:Now, as a psychiatrist, my life has been saved by police officers on more than one occasion. I have been physically attacked in hospital settings. The police have been called, and I have not died, and my colleagues have not died thanks to them. And this is Flatbush, Brooklyn, New York, and these people are black people. The Flatbush, at least the area I was in, is a predominantly black neighborhood. So, look, Americans love the police. They are a highly regarded part of society by many people, but that's not the experience for black America I have learned.Master Sergeant:“There are many things you can do in that spectrum that don't involve actively using force against a human being, which makes the process easier across the board. If I don't have to hurt somebody, the only thing that is hurting another person does for me is further endanger my Troops. "Owen Muir, M.D.:Now this makes sense to me because, having run the show in a psychiatric emergency department, where I have to protect myself, other patients, and violent people themselves from getting hurt, sometimes we use violence, but oftentimes we don't.Master Sergeant:"What started this particular instance has been four cops lynched George Floyd. One guy put his knee on the man. We don't do that to terrorists actively trying to kill us. ""George Floyd, Say His Name."Sequoiah:"It was at that point that they called in more backup and started to attack and arrest groups of gathered people from the neighborhood.”Owen Muir, M.D.:Police officers, when they're called to stand trial for the use of force, have a standard called the reasonable officer standard.I feel like I have to make it relevant for me--a white person—to watch humans being murdered by police and then people killing each other in the streets about it. There was an article I read about six months ago about yet another person being slammed to the ground, handcuffed behind their back, and suffocated to death by the police. I was shocked..that the person was white. Until I read several paragraphs down that he had schizophrenia. Oh, that's what made it okay. Reasonable officers can only be judged based on what someone would do in that moment of terror when they have to decide to use force.Sequoiah:"I was so emotionally spent and so exhausted. And then we saw marauding bands of police officers going down the street, just telling people to go home and attacking groups of people on the street.”"George Floyd, Say His Name. George Floyd, Say His Name."Owen Muir, M.D.:Police officers are represented by unions. Those unions have spent 20 years bargaining for lack of accountability to protect, in their minds, their members. This means police officers have the right to huddle and discuss their stories before speaking to prosecutors. It means many other things. But importantly, whenever any officer stands trial, the jury is instructed, per Chief Justice Rehnquist, to not use the benefit of 20/20 hindsight in judging their actions, but only what a reasonable, that is, terrified person, would do at the moment.Master Sergeant:"We have an entire job in the US military to validate whether or not we killed someone the right way."Owen Muir, M.D.:The court system is what's supposed to do that for police officers. But it doesn't; it just says, eh, it's okay.Master Sergeant:"That's an actual thing; we have entire organizational structures dedicated to the legality of murder."Owen Muir, M.D.:Killing black or brown people in America, if you're a police officer, has literally never been ruled against the law. Ever.Master Sergeant:"To not call it murder, to call it, to call it killing combatants, that's what a JAG does. Overseas, when they're deployed, they tell you whether or not you can kill this person. And sometimes, even though we can kill someone, we don't because they have a much higher value as an intelligence asset. Or for any number of other reasons. Or they're not actively shooting at us when we go get them. That happens a ton. Because sometimes, when you see 20 or 30 goons show up outside your house, breach your door with a shotgun round, rush in, and then point all their guns at you, you won't fight back. And then, okay, well, he's not shooting back at us, so we're going to take him in, and then... "Owen Muir, M.D.:You don't get to kill someone. In the U. S. military. Deployed in the field. In Afghanistan. Even if someone's a terrorist, if they're not pointing a gun at you and about to pull the goddamn trigger.“Cause one of the things I don't want to do is vilify police officers. And, and ...”Master Sergeant:"I mean, Owen, to be perfectly honest with you, You may not want to vilify police officers, but the things I've seen police officers do in the past week while they know they're being recorded are actively the actions of villains."Owen Muir, M.D.:This hit me like a ton of bricks. This is not okay, but when people call for help, and the police arrive, they deal with a crisis. A lot of those crises involve people with mental illness, and police officers are being asked to do a thing that like is a whole medical specialty. Like, I'm a psychiatrist. It was 45 000 hours of training to learn how to calm people down when upset and have experiences we don't have access to. And, if you're called to the scene of a crisis, and someone's acting in a really strange and scary way, and you have a gun. You've been told to protect yourself, don't let yourself get hurt or let this person harm you, and you know nothing bad will happen to you if you pull that trigger. You're going to pull that trigger. More often than not. And that's about a thousand times a year. You're about... God knows it doesn't even matter. The percentage of time you're more likely to be killed if you're black and mentally ill. The fact that we have a statistic for that is fucked up enough. Help isn't helpful for black America. And that's just a fact of life.”Master Sergeant:"You know, I have friends in New York who are talking about the cruelty they see in these police officers’ eyes. And what's worse, what's truly evil about this whole system is even in the throes of this violence, they're exhibiting racist and preferential behaviors towards white protesters versus black protesters. Or brown protesters. They're active, you know, taking it easier on white people because they're white. "Owen Muir, M.D.:And this is just f*****g killing me at this point. Ugh. Look, what's happening in the streets is not okay. It's not been okay for hundreds of years. And police officers are part of a system designed to keep order, and order used to mean slaves. That's just why they're there.Master Sergeant:"Things I don't even f*****g think about, man. Like, I'll go for a run or a rock at night. And I'll, I'll like, sometimes I'll go on my own, but if I don't go earlier, like, T. is like, well, I guess I'll go for a run. Like, one day, I just asked, like, why do you only run with me? Why do you only run with me? And she's like, well, it depends. We're in a quiet neighborhood in Florida, and I'm a black woman like I’m; there’s a bunch of Trump signs everywhere like I'm not going running on my own. I was like, wow, yeah, I've never even thought along those lines; I don't question my safety when I go places. I'm hyper-vigilant for a lot of other reasons, but like, there's never a question in my mind, like if someone attacks me, it's not, it's an unexpected event, I'm not expecting, That at any moment, someone might attack me for the color of my skin. Because I'm in the neighborhood."William Osei, PhD.:"Hey, I'm Dr. Will Osei.I am a postdoctoral fellow, an African American psychologist living in Bedstuy, Brooklyn. " Owen Muir, M.D.:Dr. Osei is a scholar of racism and multiculturalism.And helped me explain what it's like for the black kids I've treated at Bellevue all these years.William Osei, PhD:"The average African American, this is like... This is a fact. This is not a revelation because we now have better cell phone coverage of these crimes. I remember being in Cleveland the day following Tamir Rice being murdered in the playground. And I was working with 12-year-old boys in the Cleveland school district. And I was devastated that day, and I went into that school expecting those boys to be devastated that their schoolmate, a kid they used to play with at the playground, was just murdered. And to them, it was nothing. It was more shocking because they knew a dozen people that the police had murdered. They knew that was just the latest murder that year. It just happened to be one that rose to the national conversation, but in Cleveland that year, there were probably 30, 50 police shootings.Owen Muir, M.D.:My level of outrage at watching all of this. That's privilege too.William Osei, PhD:"Yes. "Owen Muir, M.D.:Because to understand this as anything other than the rules of engagement would be a misunderstanding. For a long time, Black America has known to watch out when you talk to the cops because they can kill you. Nothing's going to stop them if they want to. And they do. On camera. A thousand other times every year. And I wish it were as easy as saying it was a couple or even a lot of bad apples, but that is insufficient.Master Sergeant:"As far as privilege goes, I’m a combat veteran in the Ivy League. I'm an Arab Jew, but I look white enough that no one asks that question. I wear a suit, and you can't see my tattoos. And I... I can fit in anywhere from West Hampton to the slums of Bangladesh. Like, I'm good. You know what I mean? I have levels of privilege that people use to run for the presidency."Owen Muir, M.D.:But the magic of America is that white privilege runs out as soon as power wants it to. My colleague's married to a black woman.Master Sergeant:"And a huge part of this is like... It's the knowledge that I'm married to a black woman. My kids will be black, and this is like their plight. "Owen Muir, M.D.:Usually, we'd have credits now. Instead, I’m going to read these names.George Floyd, Ahmad Arbery, Brianna Taylor, Trayvon Martin, Eric Garner, Iyanna Jones. Freddie Gray, Michael Brown, Sandra Land, Walter Scott, and a kid on a playground in Cleveland named Tamir Rice. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 23m 47s | ||||||
Want analysis for the episodes below?Free for Pro Submit a request, we'll have your selected episodes analyzed within an hour. Free, at no cost to you, for Pro users. | |||||||||
| 4/7/25 |  The Scalable Depression Solution | Owen Muir, M.D. of The Frontier P This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 33m 03s | ||||||
| 4/3/25 |  Tardive Dyskinesia: Do I Have It? | Oh my. The irony is thick with this one. Your author, and sometimes scientist, Owen Scott Muir, M.D. has been doing research on Tardive Dyskinesia. And…he might have the disorder. The search function lets you search for other articles on the topic. If you are interested in treatments for psychiatric disorders that don't cause this adverse effect—a permanent movement disorder—they exist. The care we provide in New York, California, and now, South Carolina works, diligently, to advance the science of safer treatment. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 24m 34s | ||||||
| 3/18/25 |  Can Inflammation Status Predict Response to Depression Treatment? | The frontier Psychiatrists breaks down a publication on the topic of immune modulation of TMS response in depression. And Dr. Owen Muir explains what inflammation is for mental health conditions in the process. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 12m 44s | ||||||
| 3/1/25 |  The Plague Of Athens Podcast | I’ve been obsessed with the Peloponnesian War as a historical event for 20 years now. I wrote an article about it recently, and also recorded a song about it many years back.Enjoy the listen!If you like the music, there is more of it on Spotify…The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 16m 48s | ||||||
| 2/20/25 |  How Did Rapid Remission from Depression Become the New Standard of Care? | This podcast was edited on a plane ride to Japan, and the intro was recorded in a bathroom while my kids slept off the jet lag. It’s still good. I recently went down with Ben Greenzweig, the Executive Director of the non-profit Living Water Brain Treatment Center in Myrtle Beach, South Carolina. We are—right now—providing TMS treatment and, soon to be more, in a local community in Ben’s beloved home of Horry County. There are 400,000 residents and less than 30 psychiatric inpatient beds in the county. There are not enough services to meet the needs he saw in his community—so he started Living Water to help. I’ll remind readers that not only did he write an article about it, but he is also running a non-profit. Thus, consider donating.The audio from today’s podcast was recorded mainly on my phone, which I had in my pocket as I gave the talk. Please share it with friends. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 37m 18s | ||||||
| 12/15/24 |  The Mystery of Machine Gun Kelly | My readers and listeners know that this project, The Frontier Psychiatrists, is daily. Sometimes, I don't get the thing done till the end of the day. Today is one of those days. I was running on empty when it came to narrative this morning, so I decided to try to make a podcast. One of the tricky things about these more experimental days is that I don't know if the story is going to work. It's like walking a tightrope. I'll choose something— anything— to write about. And today I decide to make it even more difficult for myself, because I didn't feel like typing anything, and so I made a podcast instead. Today's was going to be about Machine Gun Kelly and being old. That's all I knew. The podcast you're about to listen to explains what happened, and the lessons I took away from the journey of trying to figure out who the heck Machine Gun Kelly is. The podcast features some of my favorite people, including Michelle Bernabe, RN , Courtny Hopen, RN, and my mom, Vita Muir. Surprisingly, it ends up featuring Drew Barrymore, and I'll let you listen to figure out how that happened. Thanks for joining me on this publication's experimental journey. I really hope you listen to the episode. It took all day to land, and I think it's good enough.Yes, the podcast was created—top to bottom— today. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 20m 54s | ||||||
| 12/9/24 | 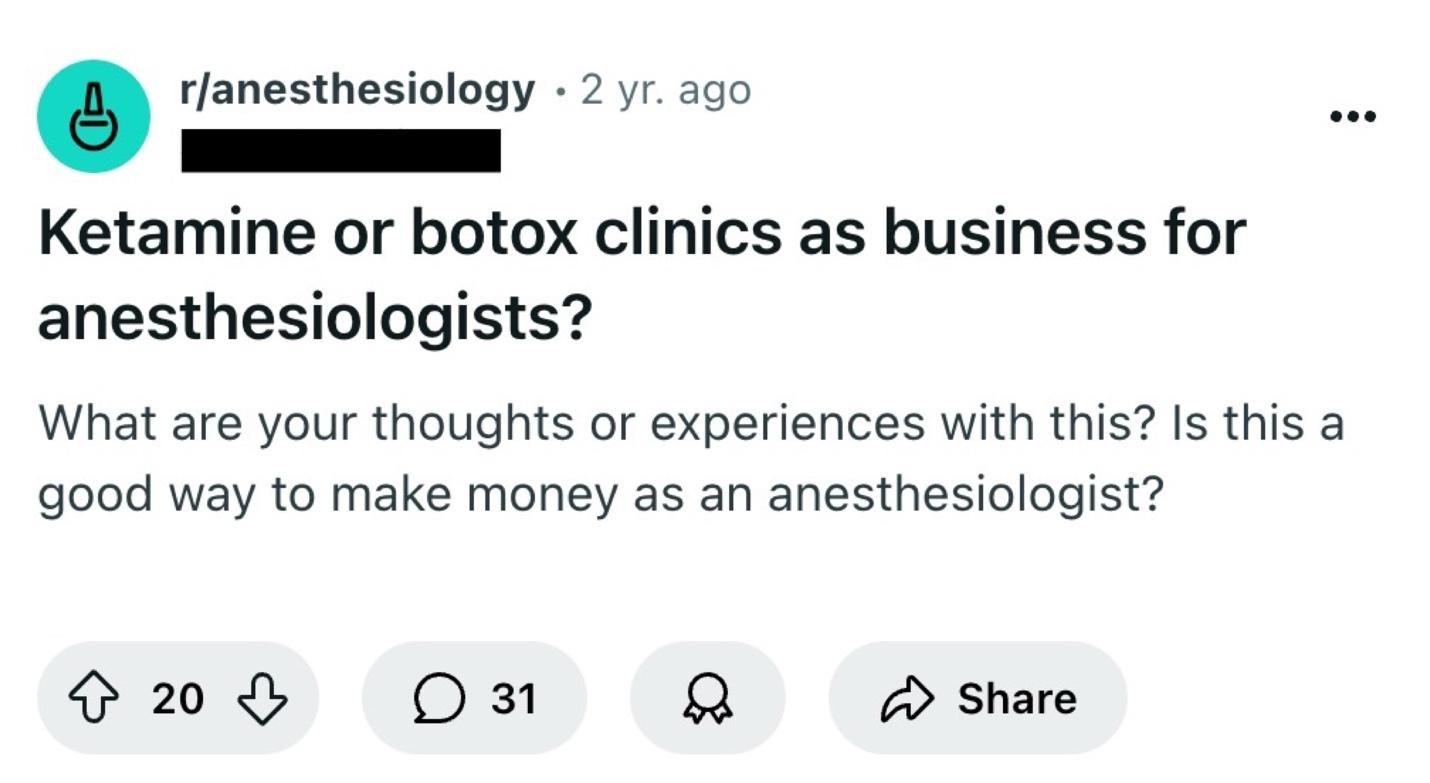 Why Ketamine Clinics Keep Closing | Today, The Frontier Psychatrists welcomes back my friend Ben Spielberg. He's been a reader for a long time and has contributed to the newsletter in the past. It was on Clinical Trial design, a perennial favorite around these parts.With only light edits, what follows is his work, narrated by me, for the Audio Version.I would invite you to the live class today on working as an out-of-network provider, but it sold out last night, so you'll have to wait for the next one. My prior article on Spravato is available here.The year is 2024. OpenAI has just launched its latest update to ChatGPT, promising more natural and less artificial-sounding language. Donald Trump has won the nomination for President of the United States. Another chain of ketamine clinics has engaged in a corporate reorganization. There is conflict in the Middle East. Are we sure that we're not living Groundhog's Day?I am the founder of Bespoke Treatment, an integrative mental health facility with multiple locations that has at times been referred to as a "ketamine clinic." I have also seen countless so-called "ketamine clinics" sell for pennies on the dollar and go bankrupt seemingly overnight. In this case, Numinus, a company that was publicly traded in Canada and owned a number of psychiatric clinics specializing in ketamine in the US and Canada, has sold its clinics to Stella (a company that has stealthily become one of the larger mental health providers in the country and is the first to bring the awesome SGB treatment to scale). It's not the first time this has happened. It's not the second, nor the third, nor even the fourth time this has happened. But yet, the common consensus is that ketamine clinics are a cheap, easy business with recurring revenue. So, what gives?Figure 1. A reddit user asking anesthesiologists if they should start a ketamine or Botox clinic for easy cash on the side. Does this make you feel gross? Should it?The Ketamine Clinic Model 101The most basic outline for a ketamine clinic is as follows: a provider rents an office space with, on average, five or so exam rooms. They buy equipment for infusions like a pump, catheter, needles, and syringes. They buy some comfortable recliner chairs. They hire a receptionist to answer phones, field patient questions, charge credit cards, and handle medical record requests. They hire a nurse to insert the IV, monitor vital signs, check blood pressure, juggle multiple patients at once, and make sure the ketamine is flowing into patients’ veins unencumbered. Two SKUs are typically offered: ketamine infusions for mood, which last approximately 40 minutes, and ketamine infusions for pain, which last for up to 4 hours. Zofran is offered for nausea, and some clinics have fun add-ons like magnesium or NAD. An average mood infusion costs around $400-$500 in a medium cost-of-living area, while mood-infusions can run up to $700 in a higher cost-of-living area. Some clinics offer package discounts if patients buy six or more upfront, which helps with cash flow for the clinic (cash now is better than cash later, of course).A Note on Scope of PracticeThe first wave of ketamine clinics was started mainly by providers who were not mental health specialists. Instead, they were owned by anesthesiologists, ER physicians, and sometimes CRNAs. These providers were especially experienced with ketamine in hospital settings, as well as setting up infusions. Psychiatrists, on the other hand, do not usually order infusions in outpatient settings, and very few had actual hands-on experience with ketamine in practice. That being said, there are a number of variations to the model above: psychiatrist-owned ketamine clinics would often prefer to use intramuscular injections in lieu of infusions, but 2-3 injections would have to be given during a single session for mood and pain sessions were out of the question. Other ways to save costs might include having an EMT do the actual injections (this is highly state-dependent), asking nurses or MAs to work the front desk, or working a full-time regular doctor job. In contrast, your nurses run the actual ketamine services via standing orders, a written document that details routine and emergent instructions for the clinic.Some clinics offer full evaluations prior to rendering treatment, but many offer a simple brief screening on the phone to check for contraindications before scheduling a patient for their first session. The clinics owned by psychiatrists have historically been a bit more thorough in terms of the initial psychiatric evaluations, given that they can actually perform initial psychiatric evaluations within their respective scope of practice. Sometimes clinics may have therapists on-site who can render ketamine assisted therapy (meaning, therapy occurring concurrently) for an additional $100-$300. Otherwise, there is not much decision-making that goes on— other than deciding on medication dosages. Most infusions start off at .5mg/kg of body weight, which is by far the most evidence-based dosage. In practice, most clinics increase dosage every session because even though ketamine is considered to be a weight-based medicine for anesthesia, there is thought to be a “sweet spot” of dosage for everyone, if one can imagine an inverted U shape curved, where the ideal dosage for each patient is at the tippity-top of the inversion. Dosage increases are highly variable depending on the clinic: some have a maximum dosage, some will only increase a certain percentage, and some may even use standardized increments (e.g., only offering dosages in increments of 50mg). A typical series of infusions is 6-8 over 3-4 weeks, followed by boosters as needed.Fool’s GoldAt first glance, the business model seems fantastic. As a cash business, there are no AR issues, no third party billing companies to deal with, and no prior authorizations to fight over. Sure, the cost is high, but it’s not that high compared to many other healthcare services. Since the benefits fade over time, a ketamine clinic has built-in recurring revenue from patients every week, month, quarter, or year – it’s like a subscription business! Ketamine is trendy and sexy; TV shows like White Lotus mention it, and ravers from the 90’s recall it with great fondness. Unlike SSRIs and psychotherapy, ketamine works for depression fast. It’s amongst the fastest treatments for depression that we have today, and there are a lot of depressed people. It can help someone out of debilitating depression in 40 minutes. It has none of the un-sexy side effects of SSRIs like sexual dysfunction, gastrointestinal discomfort, or uncontrollable sweating. Instead, it has sexy side effects: euphoria, hallucinations, and feelings of unity with the universe. Also, unlike SSRIs, it helps most people who try it. It really is an amazing treatment, and I often feel grateful that my clinic is able to offer it to patients in needFigure 2. Most business-savvy reddit user.Supply and Demand… or SomethingMood disorders disproportionately affect individuals who are of lower socioeconomic status compared to individuals with a lot of disposable income. Of course, wealthier individuals are no more immune to mental health disorders than anyone else, but the main target market that benefits most from ketamine just do not have the means to afford it. They don’t have $3,000 to burn on yet another treatment that may or may not work. Often, the patients who could really use a series of ketamine infusions cannot scrounge enough money for a single infusion, let alone a whole series and prn boosters. However, there should be enough depressed people with cash to throw around out there… right?Wait, Isn’t That A Horse Tranquilizer?Of course, ketamine clinics can find more patients via marketing and advertising. However, I’ve found that many medical doctors who see this population, like primary care providers, are not up to date with the research. When I first launched my company, I used to go door-to-door to medical buildings in Santa Monica with cookies to speak with them about advancements in interventional psychiatry. I cannot count the number of times that I was laughed out of each office; referring providers are risk-averse, and the perception of ketamine has traditionally been poor. Medical doctors would exclaim, “Of course people feel better; you’re getting them high,” and lament that I was administering a drug thought to be highly addictive. Psychotherapists, who would also be fantastic referral partners, generally refer to psychiatry, but it’s less common for them to refer to specific treatments. Nowadays, psychotherapists who are particularly invested in ketamine can sign up with venture-backed companies like Journey Clinical and render their own ketamine-assisted psychotherapy with some prescriber supervision. The issue is that despite the media attention, people with depression don’t read innovative health newsletters, nor do they review papers in scientific journals. They rely on information from their psychiatrists, medication management providers, and psychotherapists. If they are not told that this is an option for them, they won’t hear about it without ad spend. Oh yeah, and there is a major issue with ad spend: the word ketamine itself is a restricted drug term, and legitimate clinics routinely get banned from Google and Meta for mentioning it, which makes digital advertising more difficult than it would be for any other legitimate service.The Matthew Perry EffectKetamine is very desirable for some patients (unfortunately, sometimes the patients who want it most are frankly the worst candidates for it), but I’d wager that the majority of patients who need it are kind of scared of it. They want to feel good, they want relief from depression and trauma, but it’s a weird thing to do a drug that is a horse tranquilizer and also an anesthetic in a reclining chair in a medical office that tricks your brain into feeling like you’re dead for a little bit. It’s kind of far off from acupuncture and more traditional alternative medicine. There is certainly a non-zero addictive potential that needs to be carefully weighed, it’s not a particularly comfortable experience for many patients—especially those with a history of trauma—even if it helps after the experience is over. Additionally, the famous actor from the most famous show in the world, who was deemed to have a cause of death relating to ketamine, isn’t exactly helping mass adoption. Overall, this just makes marketing and advertising even more expensive, because a) the majority of referring providers are skeptical, b) patients can’t pay for it and c) patients who can pay for it are cautious.Disruptive Business ModelsIn the model I’ve described above, there are 3 sets of cost centers: rent, staff, and marketing. In some areas of the country, rent may be negligible, and in others, it is quite high. Like an owner-operated restaurant, if a clinic is owned by a company that is not a clinician, they have to find one and pay for one. Venture-backed companies like Mindbloom, Better U, and Joyous have also created entire businesses on the back of the COVID-era controlled substance waivers, whereby they send patients ketamine tablets and/or lozenges directly through the mail. Unlike the clinic model, they don’t have rent to pay, and since national marketing campaigns are often cheaper than hyper-local brick and mortar campaigns, they are able to find new patients at lower acquisition costs compared to their clinic counterparts. Some patients do extensive research before treatment and only want to find IV clinics that offer specific dosages, but many are fine with the cheapest ketamine possible, and would prefer to pay as low as $150 for an entire month compared to $3,000.Figure 3. Did you sign up for a discounted ketamine subscription on Black Friday after purchasing a new flat-screen TV?Spravato: Coming In HotJohnson & Johnson’s branded esketamine (note the prefix es) is on track to reach coveted “blockbuster status.” While it was FDA approved for Major Depressive Disorder in 2019, it took some time to catch on for a number of reasons including skepticism that the added es only added to pharma pockets and didn’t actually work, health insurance companies taking time to decide on what their medical necessity criteria should be, and social isolation due to COVID-19 being a thing. My clinic has become one of the larger Spravato providers in the Los Angeles area, and while we still offer ketamine infusions, our infusion census has decreased by over 70%. The scenario is this: a patient with severe depression comes in to see us, they’ve heard about ketamine, but they find out that Spravato is covered by insurance for a $20 copay. Maybe ketamine has slightly better efficacy (which, in my opinion, is really just a function of being able to adjust dosage). Still, patients would prefer paying a lot less money to receive almost-the-same benefits.Death By A Thousand SticksThere are a number of other issues with the model that become problematic, especially at scale. Large medical distributors like McKesson and Henry Shein have instituted CYA policies, limiting ketamine sales to licensed anesthesiologists. Medical malpractice carriers alike have followed suit, requesting detailed addendums from providers regarding their ketamine training or flat-out refusing coverage for anyone who isn’t an anesthesiologist. Since controlled substance manufacturing is directed by the DEA based on their own predictions, it’s not uncommon for ketamine to go on shortage for weeks to months at a time. There are a myriad of problems with the model of point solutions which have been detailed here already, but in short, the old adage rings true: if all you have is a hammer, everything looks like a nail, and if all you have is ketamine, everything looks like a juicy vein. But while ketamine is a highly efficacious treatment, it’s not the best treatment for everyone, and patients can become downright dysregulated after ketamine, which a clinic in this model just can’t handle adequately at scale. And ultimately, methods to do everything cheaper don’t work out that well. For example, putting multiple patients in one room may seem like a good idea, but it is ultimately not conducive to the actual ketamine experience. Any sort of vertical integration also adds an insurmountable amount of complexity, like starting to offer Spravato or TMS, because now they have to start accepting insurance, become in-network, manage billing and AR, and so on. Depending on location and the clinic set-up, they also require specialized providers onsite.Figure 4. Supply chain issues abound.Insurance IssuesSome patients try to be well-informed. They, rightly or otherwise, don’t believe everything they hear from their providers, so they call up their health insurance companies and ask. They just call the phone number on the back of the card and ask the representative if ketamine infusions are covered. Undoubtedly, the representative says yes—even though many insurance companies have published guidelines that explicitly deny any coverage for ketamine for a mental health disorder. These patients come in frustrated, distrustful of their providers and reaffirms their belief that ketamine clinics are just cash grabs. Even if one manages to obtain a coveted insurance contract for ketamine, like Ketamine Wellness Centers had with the VA, it kickstarts cashflow and complexity issues that scale should sort out, but ultimately doesn’t because of the aforementioned issues above.Overall, it is possible to have a successful ketamine clinic in 2024. Still, it isn't easy due to market conditions, the population served, and the ever-changing landscape of mental health treatment. While many successful clinics exist today, the wheels tend to start to fall off when scaling, where all of a sudden, a clinic’s reach has surpassed its captive population. Otherwise, it becomes a series of continual cost-cutting until there is nothing left to cut… save for the business itself.Ben Spielberg is the Founder and Chief Executive Officer of Bespoke Treatment, a comprehensive mental health facility with offices in Los Angeles, CA, and Las Vegas, NV. He is also a PhD Candidate in Cognitive Neuroscience at Maastricht University.For more on psychiatric medications, buy my book Inessential Pharmacology. (amazon link).For pieces by other TFP contributors, follow:Alex Mendelsohn, Michelle Bernabe, RN, @Psych Fox, Carlene MacMillan, MD, David Carreon, M.D., Benjamin Lippmann, DO, Awais Aftab, Courtny Hopen BSN, HNB-BC, CRRN, Leon Macfayden and many others! The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 18m 35s | ||||||
| 12/8/24 |  Building Trust In Clinical Trials | The Frontier Psychiatrists is a daily-enough health-themed publication. But sometimes, I just want to make a podcast. Today is one such day.Enjoy!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 10m 40s | ||||||
| 12/4/24 |  THIS IS NOT THE WAY: CEO of UnitedHealthcare Murdered in Midtown Manhattan | Today is a day of mourning. In broad daylight, in the city I love, Brian Thompson, the CEO of UnitedHealthcare’s insurance subsidiary, was murdered. According to CNN:Brian Thompson was walking toward the New York Hilton Hotel in Midtown Manhattan, dressed in a suit and tie, to attend UnitedHealthcare’s annual investor conference being held in the ballroom.A gunman, who investigators tell CNN was masked in the sub-freezing temperatures, waited for about 10 minutes before Thompson’s arrival, before opening fire from 20 feet away shooting multiple times, striking Thompson.The gunman fled, cutting through an alleyway and hopping on to a bicycle, the official told CNN. Investigators are continuing to canvas the area. Police currently believe that the suspect fled into Central Park.Brian was 50 years old. I don't know the man, personally. I do know that he was doing his job, and somebody murdered him in cold blood.This is not the way. Assassinations are not how we resolve disputes in a civil society. I get frustrated with United Healthcare, and I make fun of them for some of their decisions. This should never be mistaken for malice: these people are doing their jobs, just like the rest of us. They need to feel safe to make good decisions. They deserve to feel safe, even if they make what some might consider bad decisions. There is no level of a bad decision in a business context that gives anybody the right to put a bullet in your chest.I don't know why this masked shooter did it; I'm guessing this was somebody with a rationale of their own. We'll find out—or we won’t. But none of us should celebrate this; everyone should decry targeted violence.It's also worth noting that United Healthcare's decisions have made people tremendously angry. Your anger about a business policy isn’t an excuse to joke about someone’s murder. This is a man with a family, friends, and loved ones.This isn’t remotely funny. This isn’t ok. Mr. Thompson and all of us deserved better.Let’s all get on our knees and pray that this sort of violence leaves our cities and threatens our lives no more. We can have disputes about best practices and employment law like adults, but never, ever should we make light of the murder of a man who deserved dignity and life.Today, I stand unapologetically and without hesitation with UnitedHealthcare and its team. You are loved and deserve better. I hope and pray for justice and healing. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 3m 14s | ||||||
| 11/15/24 |  RFK (the) II Tries Out For Richard (the) III | Synopsis:Bobby, alone on the side of the road driving back to Manhattan after loading a bear carcass into his Cybertruck, reveals his intention to play the villain. He then pretends to console Donald, the first victim of this villainy. After Donald is led off toward the White House, Bobby greets Elon, who tells him that someone is very ill from an infectious disease. Bobby, once again alone onstage, outlines his plan to have Donald killed by preventable illness and to marry Lady Melania.—Act I, Scene IBobby: Now is the administration of our discontent Made glorious summer by this son of New York Real Estate, And all the regulatory burdens that loured upon our agency, In the deep bottom of the grave, buried. Now are our Houses of Congress o’erflowing with victorious representatives, Our primary battles ceased, and our districts justly called, Our stern alarums about “voter fraud” turned to merry winnings, Our dreadful attack ads to smug tweets. Grim-messaged campaigns hath chilled the f- out; And now, instead of threatening election workers with a bloody revolution To fright the souls of LibTards, Donald Capers clumsily in Laura Loomer’s chamber, But I, who am well-shaped for sportive adventures thanks to my healthy diet, And made to drink raw milk from a cool glass; I, that am built, healthy, robust, and also sexually functional To strut before a wanton ambling nymph such as Melania; I, that am curtailed of his fair proportion of the wives of others, Cheated of affairs by regulatory limits on supplements to enhance my male nature, Unengorged, under aroused, sent before my tumescence Into this bedroom scarce half ready, And that so lamely and lacking prompt virility That ladies will ask, “Are you ready?” and “Maybe this is a bad time?” as I prepare for them — Why, I, in this weak piping time of GOP dominance, Have no delight to pass away the time, Unless to see my manly shadow in the sun And be impressed by my physique. And therefore, since I cannot prove a lover To entertain these fair, well-spoken days, I am determined to prove a villain, and hate the regulations that might limit my consumption of supplements and medicines to enhance the idle pleasures of these days. Plots have I laid, regulations dangerous, By drunken prophecies, libels, and appointments to agencies that I have no business running, To set my friend Donald and Elon In deadly hate, the one against the other; And if Elon be as Bold and Ambitious As I am subtle, false, and treacherous, This day, should Donald be held up About an Infowars story, reposted on Breitbart and OAN, that says that “RFK” Of JFK’s heirs, the most important appointment, shall be. Dive, thoughts, down to my soul. Here Donald Comes! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 3m 54s | ||||||
| 11/13/24 | 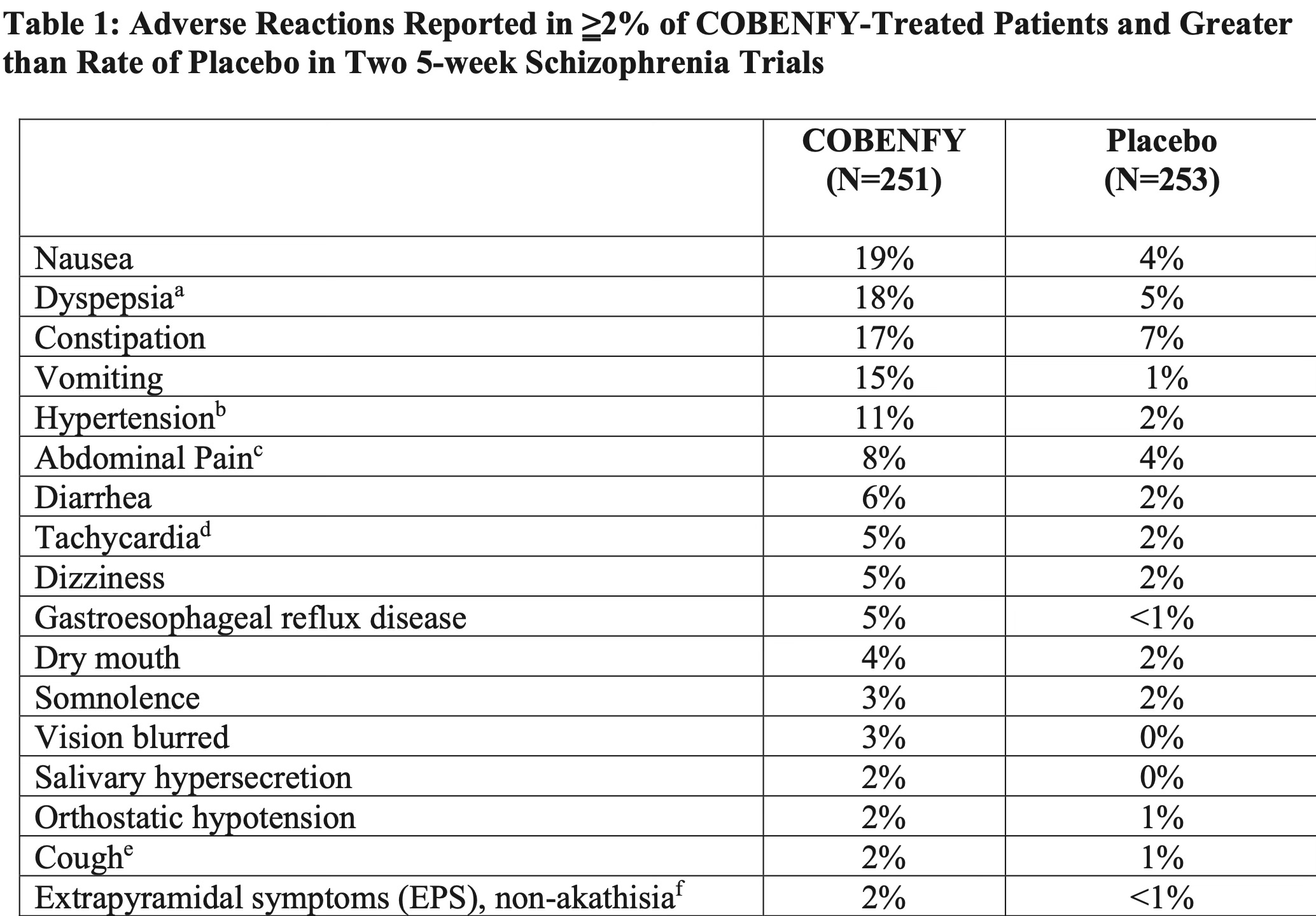 Cobenfy | The path from xanomeline to the brand name treatment named Cobenfy was a long one. Cobenfy is FDA-approved for the treatment of Schizophrenia. Here is the literal label:COBENFY is a combination of xanomeline, a muscarinic agonist, and trospium chloride, a muscarinic antagonist, indicated for the treatment of schizophrenia in adults.To people who haven't yet read my book Inessential Pharmacology, (Amazon Affiliate Link), I will highlight that this is approved as a monotherapy. That means it can be prescribed as the only drug for people with Schizophrenia.It has a completely different mechanism from every other antipsychotic. All the others block or modulate dopamine to some degree. Those are the variety of drugs I have written about, in less than glowing terms, in some cases.These are medicines that lead to obesity and early death (particularly in youth on Medicaid). I have argued they should never be used as augmentation agents.I argue, in fairness, a lot of things. One of the things I have argued about regularly is that individuals, particularly those suffering from devastating illnesses like schizophrenia, deserve treatment that works. That same treatment best if it doesn't harm the person also. The problem with antipsychotic medication is that they regularly harm the people who take them.Finally, we have a new drug that is helpful for individuals with schizophrenia and less harmful in terms of catastrophic adverse events like massive weight gain and tardive dyskinesia.What are the adverse effects for Cobenfy? Yes, those used to be called side effects.It's overwhelmingly causing problems related to nausea or other predictable anticholinergic side effects in the peripheral nervous system, especially the G.I. tract. I'm not saying it doesn't suck. I'm not saying it doesn't have side effects. But what you don't see there is massive weight gain. What you don't see there is permanent movement disorders. Does it work? In short, yes, it works. Nothing works fabulously well in schizophrenia yet, but it's not a slouch treatment, and it's not worse than existing drugs at least in the people they already studied (again, from their submission to the FDA):It's the first not me-too for schizophrenia, since clozapine. It's got a restricted range of side effects that are annoying, but not life-threatening. Will we discover more at large scale? Probably.Bristol Meyers Squibb is not done yet. They are going to be bringing this drug to bipolar disorder, and other conditions. Let's reduce the risk of early death from dopamine blocking medications for everyone for whom that would be beneficial.I'm at a conference, so I'll keep this one concise, because I'm writing it on my phone. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 4m 37s | ||||||
| 10/26/24 |  Doctors of Scale | I was at AACAP and sat down with Dr. Sood, a colleague, and we had a chat about investing, goal setting, venture scaleable businesses, and private equity, and we had some fun at the expense of Red Lobster in the process. I hope my colleagues enjoy the listen!Prior articles on the topic include What If We Didn’t Blow The Horn, Private Equity Sucks at Running Business of Medicine, and more. Thanks for reading and listening, and Ashwin for joining me! This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 35m 24s | ||||||
| 10/5/24 |  The Culture of Burnout | This Podcast is a recording of departmental grand rounds presented at the Medical University of South Alabama pre-pandemic on burnout. It references a long legal back and forth I’d put up with. That has led to, last year, our legal team filing a defamation lawsuit and, this week, a request for an injunction. It’s more burnout than when I did the talk. I hope it’s still a source of sassy wisdom about what physicians must do to keep their heads in the game, care for patients, and respond with sense and compassion. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 40m 59s | ||||||
| 9/22/24 |  Why Bipolar Depression Gets Worse In The Fall with Dr. Owen Muir, M.D. | The Frontier Psychiatrists is a daily health-themed newsletter. My dear friend Courtny —who recently penned an awesome guest post— reminded me that Fall is here. And with it, seasonal changes in mood for those with Bipolar Disorder. I’ve written about having bipolar disorder before, in a letter to that disorder. I’ve written about how important sleep is to not die. I’ve even written about this specific topic—circadian rhythm changes in bipolar illness, in a prior article here. But who has the time to read anymore? Isn’t there a video or podcast I can view without having to read all those linked articles? Yes, now there is. It’s here, now, for you, my dear subscribers. I’ve got music on Spotify! I even have a book on Amazon…(affiliate link). Oh, and another book of poetry. And a therapy manual. Thanks for reading, viewing, and listening. Oh, and…50% of subscriptions to help you cope with depressing changes in lighting. A special discount is available to celebrate fall by clicking here!The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 7m 08s | ||||||
| 9/18/24 |  Infidelity: A Failure of Mentalizing? | This newsletter is quite the multi-media shop. It gave me a new tool here on Substack, and I’ll use it less-than-polishedly. I wrote a column earlier this week on infidelity, which seemed to strike a chord. This video experiment was created in response to reader feedback on that piece of writing. It’s a new format for me and far from perfect. Let me know if you dig it anyway.Remember—I’ve got music on Spotify!I’m broadly not very talented in a wide range of media.The Frontier Psychiatrists is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. This is a public episode. If you'd like to discuss this with other subscribers or get access to bonus episodes, visit thefrontierpsychiatrists.substack.com/subscribe | 5m 19s | ||||||
Showing 25 of 102
Pitch Fit is a Pro feature
See how bookable this show is for guests, which brands already advertise, the per-episode ad value, and the best-fit guest and sponsor profile. The numbers are blurred on the free plan.
How readily this show books outside guests like you.
How proven this show is for host-read sponsorships.
For Guests
ProFor Advertisers
ProUpgrade to Pro to unlock guest cadence, sponsor categories, fit scores, and per-episode ad value for this show.
Chart Positions
2 placements across 1 market.
Chart Positions
2 placements across 1 market.